Vision Rehabilitation: Introduction
Vision loss reduces the ability to cope with daily living activities, and affects the safety and quality of life. In developed countries, and increasingly in developing countries, the majority of irreversible vision loss occurs in the elderly and will represent an ever increasing part of ophthalmic practice (see Chapter 20). Unfortunately, many patients and caregivers still consider vision loss as an inevitable result of aging and often do not seek the help that is available. It is the task of the ophthalmologist to tell them that even if “nothing can be done” about many of the causes of vision loss, “much can be done” about its consequences. This chapter will deal with ways to alleviate the consequences of vision loss through comprehensive rehabilitation (also see Chapter 24).
Stages of Visual Processing
Vision is a complex, multi-stage process. Dysfunction of the different stages causes different problems and requires different solutions.
The first stage is the optical process that puts an image of the outside world on the retina. This stage can be disrupted by refractive errors or media opacities, such as cataract. A good tool to evaluate this stage is visual (letter chart) acuity which measures the MAgnification Requirement (MAR) relative to the 20/20 reference standard. (MAR is usually known as minimum angle of resolution.) Magnification devices (see Chapter 24) are the natural choice to counteract this type of vision loss.
The second stage is the receptor stage that translates the optical image into neural impulses. If this stage is defective, vision is disrupted in a different way. A blind spot in the central retina (central scotoma) may necessitate shifting fixation to a less central retinal area (the preferred retinal locus, PRL) where the receptor mosaic is less dense. This causes reduced visual acuity, which can be counteracted by magnification (see Chapter 24). However, visual acuity tells only part of the story, since the condition at the PRL tells us nothing about the condition of the surrounding retina. Since normal vision involves constant eye movements, the object of attention may move in and out of the scotoma. This scotoma interference is not quantified by visual acuity, although it may be apparent during testing, and cannot be remedied by magnification devices. The patient needs training and practice to improve fixation stability. This may be provided by occupational therapists or vision rehabilitation specialists, but it is up to ophthalmologists to recognize the need for this training and make the appropriate referral.
The third stage is that of neural processing. This process starts in the inner retina and proceeds via the visual cortex to higher cortical centers, where it eventually gives rise to visually guided behavior. This stage is undoubtedly the most complex and awareness of vision problems related to the processing of visual information is increasing, such as the perceptual consequences of traumatic brain injury (TBI) and cerebro-vascular accidents (CVAs), and in children the importance of the entity of cerebral (cortical) visual impairment (CVI). Relevant information needs to be brought to the attention of practicing ophthalmologists, and parents and educators need to be made more aware of compensatory techniques. Some cerebral defects produce obvious impairment of visual acuity and visual field. More subtle defects may exist in the presence of normal visual function on standard clinical testing. A patient with optical or retinal problems may stumble over a curb because of lack of contrast, whereas a patient with cerebral injury may be able to detect the change in contrast but unable to decide whether this is a line on the ground or the edge of a step. In this case, vision enhancement (better illumination, contrast) will not help and vision substitution, for example a cane to tactically determine the step, may be more appropriate. Visual acuity is not a good measure of processing problems, and training is the main rehabilitative option. At the higher cerebral levels the information flow is no longer exclusively visual, but is integrated with information from other sources. Normally this integration is continuous and seamless. It only reaches our awareness if information from two sources is inconsistent and causes symptoms such as motion sickness.
Aspects of Vision Loss
Since vision provides about one-half of all the input to the brain, it is no surprise that vision loss, whether minor or severe, can affect almost all aspects of life, and the complex phenomenon of vision cannot be captured from a single point of view. A convenient framework to discuss the various impacts of vision loss is by considering four aspects of visual functioning, structure, function, abilities, and consequences (Figure 25–1).
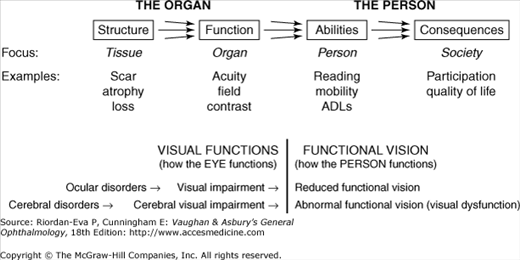
Structural changes, such as scarring, degeneration, and atrophy that are apparent on macroscopic and microscopic examination of tissue, do not necessarily indicate function, which is assessed by clinical tests, including visual acuity, visual field, and contrast sensitivity. In turn, this does not necessarily gauge the patient’s ability to perform specific tasks, such as reading, getting around, recognizing faces, or undertaking activities of daily living. Occupational therapists and other rehabilitation professionals use all this information to work with patients and teach them how their residual vision can be used most effectively. In addition, the patient’s participation in society and quality of life need to assessed.
Structure and function contribute to visual functions, which reflect the function of the visual system as an organ of the body, whereas how the person functions in vision-related activities reflects functional vision, which reflects how the patient functions as a person. Ophthalmology is well versed in analyzing the former, but the ultimate goal of all ophthalmic interventions should be to improve the quality of life, an aspect of the latter that often receives inadequate attention. Ophthalmic care, including in textbooks, traditionally prioritizes visual function, whereas for patients functional vision is more important, but the process is flexible and bi-directional such that intervention can be effective at all stages (Figure 25–2).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


