Lens: Introduction
The crystalline lens is a remarkable structure that contributes to focusing of images on the retina. It is positioned just posterior to the iris and is supported by zonular fibers arising from the ciliary body and inserting onto the equatorial region of the lens capsule (see Figure 1–12). The lens capsule is a basement membrane that surrounds the lens substance. Epithelial cells near the lens equator divide throughout life and continually differentiate into new lens fibers, so that older lens fibers are compressed into a central nucleus; younger, less-compact fibers around the nucleus make up the cortex. Because the lens is avascular and has no innervation, it must derive nutrients from the aqueous humor. Lens metabolism is primarily anaerobic owing to the low level of oxygen dissolved in the aqueous.
The eye is able to adjust its focus from distance to near objects because of the ability of the lens to change shape, a phenomenon known as accommodation. The inherent elasticity of the lens allows it to become more or less spherical depending on the amount of tension exerted by the zonular fibers on the lens capsule. Zonular tension is controlled by the action of the ciliary muscle, which, when contracted, relaxes zonular tension. The lens then assumes a more spherical shape, resulting in increased dioptric power to bring nearer objects into focus. Ciliary muscle relaxation reverses this sequence of events, allowing the lens to flatten and thus bringing more distant objects into view. As the lens ages, its accommodative power is gradually reduced as lens elasticity decreases.
Physiology of Symptoms
Symptoms associated with lens disorders are primarily visual. Presbyopic symptoms are due to decreased accommodative ability with age and result in diminished ability to perform near tasks. Loss of lens transparency (cataract) results in blurred vision (without pain) for both near and distance. If the lens is partially dislocated (subluxation) due to congenital, developmental, or acquired causes, visual blur can be due to a change in refractive error. Complete dislocation of the lens from the visual axis results in an aphakic refractive state; severely blurred vision results from loss of over one-third of the eye’s refractive power, the majority still being provided by the curvature of the cornea.
Cataract
A cataract is any opacity in the lens. Aging is the most common cause, but many other factors can be involved, including trauma, toxins, systemic disease (such as diabetes), smoking, and heredity. Age-related cataract is a common cause of visual impairment. Cross-sectional studies place the prevalence of cataracts at 50% in individuals aged 65–74; the prevalence increases to about 70% for those over 75.
The pathogenesis of cataracts is not completely understood. However, cataractous lenses are characterized by protein aggregates that scatter light rays and reduce transparency. Other protein alterations result in yellow or brown discoloration. Additional findings may include vesicles between lens fibers or migration and aberrant enlargement of epithelial cells. Factors thought to contribute to cataract formation include oxidative damage (from free radical reactions), ultraviolet light damage, and malnutrition. No medical treatment has been found that will retard or reverse the underlying chemical changes that occur in cataract formation. However, some recent evidence suggests a protective effect from dietary carotenoids (lutein), but studies evaluating the protective effect of multivitamins have yielded conflicting results.
A mature cataract is one in which all of the lens substance is opaque; the immature cataract has some transparent regions. If the lens takes up water, it may become intumescent. In the hypermature cataract, cortical proteins have become liquid. This liquid may escape through the intact capsule, leaving a shrunken lens with a wrinkled capsule. A hypermature cataract in which the lens nucleus floats freely in the capsular bag is called a morgagnian cataract (Figure 8–1).
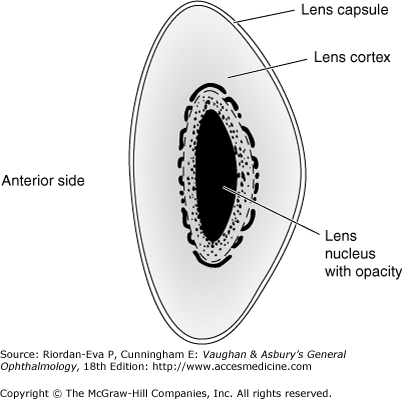
Figure 8-1.
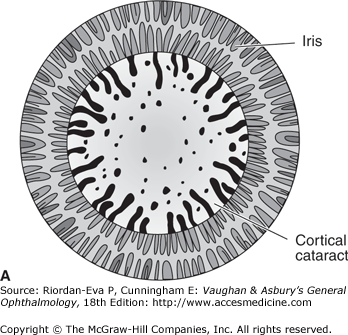
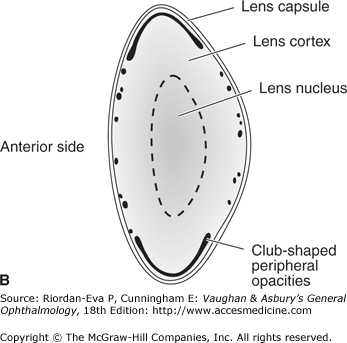
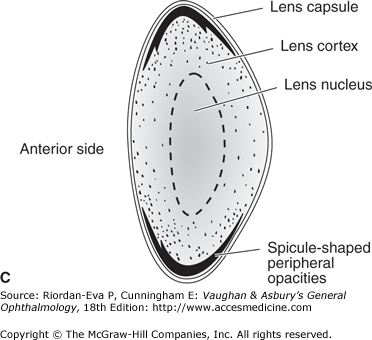
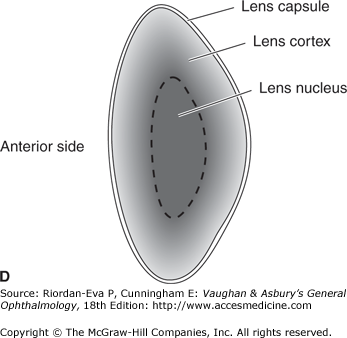
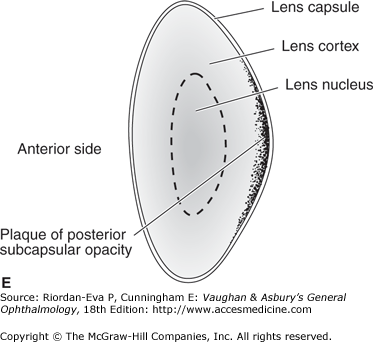
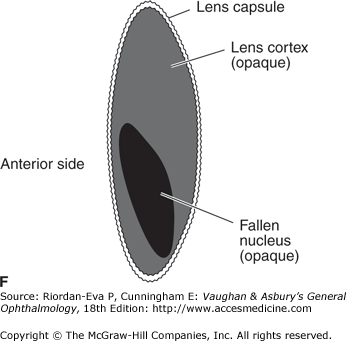
Age-related cataract. A and B: “Coronary” type cortical cataract (frontal and cross-sectional views): club-shaped peripheral opacities with clear central lens; slowly progressive. C: “Cuneiform” type cortical cataract: peripheral spicules and central clear lens; slowly progressive. D: Nuclear sclerotic cataract: diffuse opacity principally affecting nucleus; slowly progressive. E: Posterior subcapsular cataract: plaque of granular opacity on posterior capsule; may be rapidly progressive. F: “Morgagnian” type (hypermature lens): the entire lens is opaque, and the lens nucleus has fallen inferiorly.
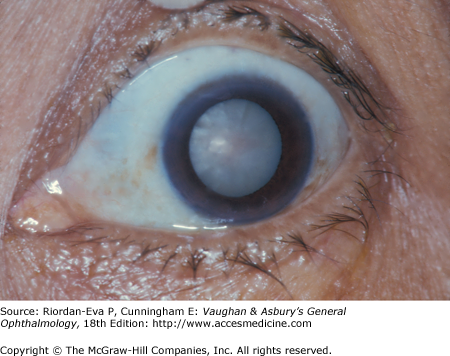
Most cataracts are not visible to the casual observer until they become dense enough to cause severe vision loss. The ocular fundus becomes increasingly more difficult to visualize as the lens opacity becomes denser, until the fundus reflection is completely absent. At this stage, the cataract is usually mature, and the pupil may be white.
The clinical degree of cataract formation, assuming that no other eye disease is present, is judged primarily by the patient’s symptoms and the visual acuity. Generally speaking, the decrease in visual acuity is directly proportionate to the density of the cataract. However, some individuals who have clinically significant cataracts when examined with the ophthalmoscope or slitlamp see well enough to carry on with normal activities. Others have a decrease in visual acuity out of proportion to the degree of lens opacification. This is due to distortion of the image by the partially opaque lens. The Cataract Management Guideline Panel recommends reliance on clinical judgment combined with visual acuity as the best guide to the appropriateness of surgery but recognizes the need for flexibility, with due regard to a patient’s particular functional and visual needs, the environment, and other risks, all of which may vary widely.
Age-Related Cataract
The normal condensation process in the lens nucleus results in nuclear sclerosis after middle age. The earliest symptom may be improved near vision without glasses (“second sight”). This occurs from an increase in the refractive power of the central lens, creating a myopic (nearsighted) shift in refraction. Other symptoms may include poor hue discrimination or monocular diplopia. Most nuclear cataracts are bilateral but may be asymmetric.
Cortical cataracts are opacities in the lens cortex. Changes in the hydration of lens fibers create clefts in a radial pattern around the equatorial region. They also tend to be bilateral, but they are often asymmetric. Visual function is variably affected, depending on how near the opacities are to the visual axis.
Posterior subcapsular cataracts are located in the cortex adjacent to the posterior capsule. They tend to cause visual symptoms earlier in their development owing to involvement of the visual axis. Common symptoms include glare and reduced vision under bright lighting conditions. This lens opacity can also result from trauma, corticosteroid use (topical or systemic), inflammation, or exposure to ionizing radiation.
Age-related cataract is usually slowly progressive over years, and death may occur before surgery becomes necessary. If surgery is indicated, lens extraction improves visual acuity in over 90% of cases. The remainder of patients either has preexisting retinal damage or, in rare cases, develop serious postsurgical complications that prevent significant visual improvement, for example, glaucoma, retinal detachment, intraocular hemorrhage, or infection.
Childhood Cataract
Childhood cataracts are divided into two groups: congenital (infantile) cataracts, which are present at birth or appear shortly thereafter, and acquired cataracts, which occur later and are usually related to a specific cause. Either type may be unilateral or bilateral.

About one-third of childhood cataracts are hereditary, while another third are secondary to metabolic or infectious diseases or associated with a variety of syndromes. The final one-third results from undetermined causes. Acquired cataracts arise most commonly from trauma, either blunt or penetrating. Other causes include uveitis, acquired ocular infections, diabetes, and drugs.



