Orbit: Introduction
Orbital disease usually arises within the orbit or by spread from adjacent structures, particularly the paranasal sinuses. The etiology may be inflammatory, due to infection; neoplastic, either benign or malignant and arising from bone, muscle, nerve, blood vessels, or connective tissue; or due to vascular anomalies, including arteriovenous malformations and arterial fistulas. Orbital lesions may also be due to metastatic tumors. Thus, orbital disease may be due to serious and sometimes life-threatening entities.
An increase in orbital contents results in displacement of the globe. Since the orbit has rigid bony walls except anteriorly (see Chapter 1), such displacement usually manifests predominantly as forward protrusion of the globe (proptosis), which is the hallmark of orbital disease. Swelling within the muscle cone displaces the globe directly anteriorly (axial proptosis), whereas swelling outside the muscle cone will also cause sideways or vertical displacement (non-axial proptosis).
Bilateral involvement generally indicates systemic disease, such as Graves’ disease. The term “exophthalmos” is often used when describing proptosis associated with Graves’ disease.
Pulsating proptosis may be due to carotid-cavernous fistula, arterial orbital vascular malformation, or transmission of cerebral pulsations due to a defect of the superior orbital roof, as in the sphenoid dysplasia of type 1 neurofibromatosis. Proptosis that increases on bending the head forward or with Valsalva’s maneuver is a sign of venous orbital vascular malformation (orbital varices) or meningocele. Intermittent proptosis may be the result of a sinus mucocele. The Hertel exophthalmometer (see Chapter 2) is the standard method of quantifying the magnitude of proptosis. Serial measurements are most accurate if performed by the same individual with the same instrument. Pseudoproptosis is apparent proptosis in the absence of orbital disease. It may be due to high myopia, buphthalmos, or lid retraction.
Proptosis does not impair vision unless there are corneal changes due to exposure, but the orbital process itself, particularly if it arises from, involves, or compresses the optic nerve, or if it causes compression of the globe, resulting in distortion of the retina and possibly elevation of intraocular pressure, may impair vision. A relative afferent pupillary defect (RAPD) or impairment of color vision may identify optic nerve dysfunction before there is significant reduction of visual acuity.
Limitation of ocular movements resulting in diplopia (double vision) may be due to direct involvement of the extraocular muscles, interference with their mechanisms of action, or dysfunction of the oculomotor, trochlear, or abducens nerves. Pain may occur as a result of rapid expansion, inflammation, or infiltration of sensory nerves.
Disease involving the superior orbital fissure produces a characteristic combination of diplopia, resulting from disturbance of function of the oculomotor, trochlear, and abducens nerves, corneal and facial anesthesia (ophthalmic division of trigeminal nerve), and possibly proptosis, known as the superior orbital fissure syndrome. Lesions at the orbital apex also result in optic nerve dysfunction (orbital apex syndrome). (In the cavernous sinus syndrome, there is diplopia and trigeminal dysfunction, potentially involving all three divisions. There may be proptosis due to venous congestion but not optic nerve dysfunction.)
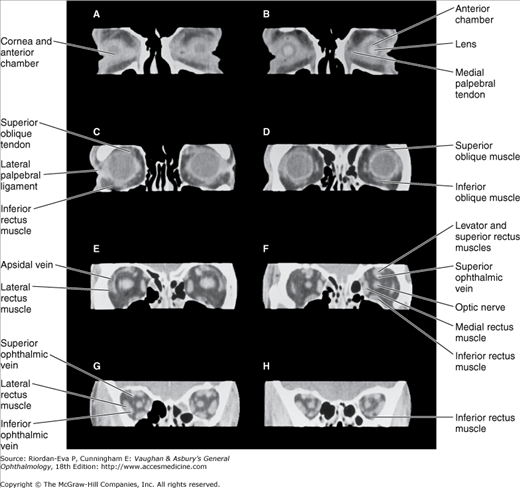
Imaging by computed tomography (CT) (Figures 13-1 and 13-2) was a major advance in orbital diagnosis. Due to continued improvement in resolution quality, rapidity of scanning, and multi-planar imaging with manipulation of images to produce three-dimensional reconstructions, it retains an important role. Magnetic resonance imaging (MRI) provides additional information on changes within soft tissues and the optic nerve but is less useful for bony changes. It is contraindicated in the presence of a ferrous intraorbital or intracranial foreign body.

The use of ultrasonography in the diagnosis of orbital disease has largely been supplanted by CT and MRI. Although it is a noninvasive and inexpensive form of imaging, its usefulness in both A and B mode is limited to the anterior portion of the orbit. It is of greatest value in the hands of the clinician-ultrasonographer capable of interpreting “real-time” images. It provides a noninvasive method of diagnosing carotid artery–cavernous sinus fistula (see later in the chapter).
Venography is rarely useful in defining the extent of orbital venous disease. Although the diagnosis can be made by MRI, contrast injection into the orbital veins via a scalp vein can sometimes reveal the presence of varices that have escaped detection by CT.
Selective carotid (catheter) angiography with bone subtraction is sometimes necessary to diagnose orbital vascular disorders. In carotid artery–cavernous sinus fistula, CT angiography may provide sufficient detail for diagnosis but catheter angiography is required to delineate the extent of involvement and for treatment by embolization.
Plain x-rays may be sufficient for initial diagnosis of orbital fractures. However, the thin walls of the orbit are difficult to visualize even with tomography, and CT with three-dimensional reconstructions is usually needed to determine the extent of injury, as well as for preoperative and possibly intraoperative planning of surgical reconstruction. CT will also show orbital soft tissue injury and hemorrhage, and may identify ocular damage, including globe rupture, intraocular hemorrhage, and lens dislocation. Dacryocystography and radionuclide scanning can be helpful in localizing the site of lacrimal obstructions.
Fine-needle aspiration biopsy is an invasive procedure that has proved very useful in orbital diagnosis. Cytology specimens can be aspirated from a lesion, the exact location of which is determined by CT. Cytopathology can be inconclusive but is often invaluable.
Diseases & Disorders of the Orbit
Graves’ ophthalmopathy is a syndrome of clinical and imaging abnormalities caused by deposition of mucopolysaccharides and infiltration with chronic inflammatory cells of the orbital tissues, particularly the extraocular muscles. It usually occurs in association with autoimmune hyperthyroidism (Graves’ disease), but exactly the same disease process can occur in association with autoimmune hypothyroidism (Hashimoto’s thyroiditis); thyroid dysfunction due to amiodarone; thyroid antibodies (antimicrosomal (thyroperoxidase) or antithyroglobulin antibodies, or thyroid-simulating immunoglobulins) without thyroid dysfunction; and occasionally no clinical or laboratory evidence of thyroid dysfunction and no thyroid antibodies, even on long-term follow-up. It is thought to be an autoimmune disease but which antigens and antibodies are important in its pathogenesis remains uncertain. It is associated with other autoimmune diseases, including myasthenia gravis. It is exacerbated by cigarette smoking and radioiodine therapy. (Graves’ ophthalmopathy or orbitopathy, dysthyroid ophthalmopathy or orbitopathy, and (dys)thyroid eye disease or orbital disease are interchangeable terms.)
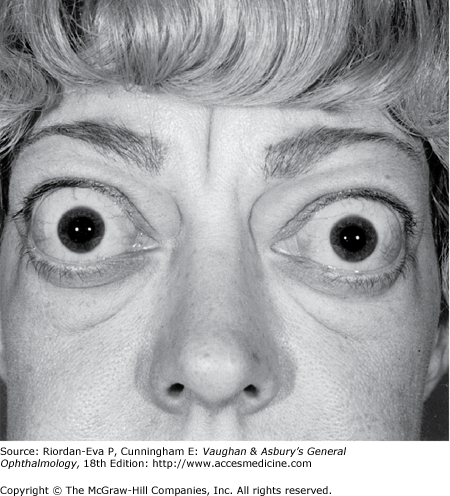
Some degree of ophthalmopathy, usually mild and typically including upper eyelid retraction, occurs in a high percentage of hyperthyroid patients. Severe ophthalmopathy with marked proptosis and restricted motility occurs in about 5% of cases of Graves’ disease (Figure 13–3).
Graves’ ophthalmopathy is the most common cause of unilateral or bilateral proptosis in adults or children. The accompanying upper eyelid retraction, manifesting as disproportionately greater exposure of sclera superiorly than inferiorly, and lid lag, manifesting as impaired descent of the upper eyelid on downward gaze, distinguishes it from other causes of proptosis.
Ocular surface discomfort is very common in all stages of the disease, in some cases due to superior limbic keratoconjunctivitis (see Chapter 5). Incomplete eyelid closure (lagophthalmos) results from proptosis and lid retraction, and corneal exposure may be present even in mild cases. Ptosis in association with thyroid ophthalmopathy is usually due to coexistent myasthenia gravis, which may also contribute to ocular motility disturbance.
The extraocular muscle involvement of thyroid ophthalmopathy begins with lymphocytic infiltration and edema of the rectus muscles, typically the inferior and medial recti. The inflamed muscles may become fibrotic and permanently restricted. Diplopia usually begins in the upper field of gaze. All extraocular muscles may eventually be involved, and there may be no position of gaze free of diplopia. Tethering of the inferior recti results in elevation of intraocular pressure on upgaze, or in severe cases even on looking straight ahead.
If the extraocular muscles become markedly enlarged (Figure 13–4), there may be compression of the optic nerve at the orbital apex, not necessarily accompanied by significant proptosis. Early signs include an afferent pupillary defect and impairment of color vision, followed by reduction of visual acuity. Blindness is liable to occur if compression is unrelieved.
Figure 13-4.
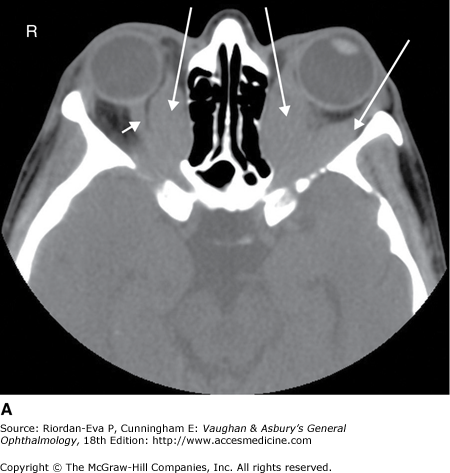
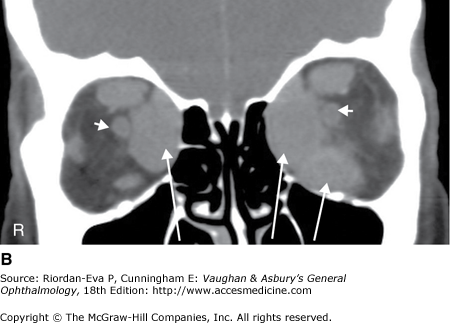
CT scan of Graves’ ophthalmopathy. A: Axial section showing markedly enlarged medial recti and left lateral rectus (arrows) and distortion of right optic nerve (arrowhead). B: Coronal section showing optic nerves (arrowheads) and markedly enlarged medial recti and left inferior rectus (arrows).
Management should be multidisciplinary. An endocrinologist should manage the thyroid status, optimal control being crucial to ameliorating the orbital disease. If hyperthyroidism cannot be controlled by drug therapy, thyroid surgery is preferable to radioiodine therapy. Whether thyroid surgery improves ophthalmopathy is uncertain. Radioidone therapy is relatively contraindicated and prophylactic steroid therapy needs to be considered if it needs to be administered. Cigarette smoking should be discouraged.
Ocular surface problems, including exposure keratitis, can usually be controlled with topical lubricants. Compressive optic neuropathy, or proptosis with severe exposure keratitis uncontrolled by lubricants, requires emergency treatment, initially with high-dose systemic steroids (oral prednisolone 80–100 mg/day or intravenous methylprednisolone therapy 1 g/day for 3 days repeated weekly for 3 weeks). If this is unsuccessful, either acutely or in the long term, including due to steroid complications, surgical decompression of the orbit is usually performed. Several techniques have been devised using external or transnasal endoscopic approaches. All aim to expand the orbital volume by removal of the bony walls, usually the orbital floor, medial wall, and possibly lateral wall, with incision of the orbital periosteum. There is a risk of causing or exacerbating diplopia and a lesser risk of orbital infection. Orbital radiotherapy may be an effective alternative in patients unsuitable for surgery but should be avoided in diabetics with retinopathy. Exposure keratitis due to severe proptosis may respond to lateral tarsorrhaphy.
Whether oral corticosteroids (prednisone up to 60 mg/day), with or without additional immunosuppressants, or orbital radiotherapy should be used in active disease not complicated by optic neuropathy or severe corneal exposure is controversial. Systemic steroids commonly result in improvement in symptoms, but the potential for complications limits their long-term use. Pulsed high-dose intravenous steroids appear to be more effective with fewer adverse effects than long-term oral therapy.
Eyelid retraction is often more disturbing than proptosis—both functionally, because of exposure keratitis, and cosmetically. Surgical orbital decompression may improve lid retraction, but correction of the retraction by lid surgery is safer and camouflages proptosis to some extent. The upper and lower lid retractors (aponeurosis and sympathetic muscles) can be lengthened by inserting a spacer such as eye bank sclera. Small amounts (2 mm) of lid retraction can be corrected by disinserting the retractors from the upper tarsal border. Once the ophthalmopathy is inactive, surgical orbital decompression can be performed for cosmetically unacceptable proptosis, but the risks of surgery need to be borne in mind.
Double vision may not be sufficiently bothersome to require treatment. While the ophthalmopathy is active, prisms or occlusion may be helpful. Strabismus surgery should not be undertaken until the ophthalmopathy is inactive and the ocular motility disturbance has been stable for at least 6 months. Tight muscles, usually inferior and medial recti, are recessed using adjustable sutures. Most patients can achieve at least a small area of binocular single vision in a useful position of gaze. Torsional diplopia, the result of oblique muscle involvement, complicates management. Botulinum toxin is rarely helpful in the acute or chronic stages of the disease. Some patients have intractable diplopia despite all attempts at correction.
A frequent cause of proptosis in adults and children is inflammatory pseudotumor. (The term “pseudotumor” was adopted to indicate a non-neoplastic process that produces the sentinel sign of an orbital neoplasm, ie, proptosis.) In some cases it is due to vasculitis, most commonly Wegener’s granulomatosis, possibly in its limited form that may not be associated with positive serum antineutrophil cytoplasmic antibodies (ANCA). The inflammatory process can be diffuse or localized, specifically involving any orbital structure (eg, myositis, dacryoadenitis, superior orbital fissure syndrome, or optic perineuritis) or cell type (eg, lymphocytes, fibroblasts, histiocytes, and/or plasma cells). There may be extension to involve the cavernous sinuses and intracranial meninges. Onset is usually rapid, and pain is often present.
Pseudotumor is usually unilateral; when both orbits are involved, it is more often a manifestation of vasculitis. The differential diagnosis includes Graves’ ophthalmopathy and orbital lymphoma.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


