Causes and Prevention of Vision Loss: Introduction
Causes of Vision Loss
Vision loss has significant consequences. Differentiating between different degrees of vision loss is important, because the demands for medical, social, and rehabilitative interventions vary.
Vision loss has been defined in many different ways, determined by the intended purpose but resulting in many terms that may not be consistent with one another. Whereas to the lay person it implies complete loss of vision, the term “blindness” is often used for individuals who have significant and useful residual vision, an extreme example being the use of the term “color blindness” for individuals with mild color vision deficiency. “Industrial blindness,” a term from the early 19th century, may be used to describe the impact on employability. “Automobile blindness” may be used to indicate that the individual does not meet the requirements for a driver’s license. “Legal blindness” is used in the United States for those who meet various legal requirements for benefits.
An important challenge is categorizing the broad range of vision loss. The eighth revision of the International Classification of Diseases (ICD-8) recognizes only two categories of vision: Sighted and Blind. In the 1970s the International Council of Ophthalmology (ICO) worked with the World Health Organization (WHO) to define three major categories in the US adaptation of the ninth revision (ICD-9-CM): Normal Vision, Low Vision, and Blindness. ICD-9 and ICD-10 do not utilize the first category.
The ICD major categories are now used in almost all population surveys, with the WHO definitions (ICD-9/ICD-10) usually having been used for surveys aimed at the detection of eye disease. Low vision is defined as best-corrected visual acuity less than 20/70 (6/18, 0.3) but equal to or better than 20/400 (3/60, 0.05) and blindness is defined as visual acuity less than 20/400, or maximum diameter of visual field 20° or less in the better eye. To describe how people live their lives, the WHO has subsequently recommended categorization according to visual acuity with presenting correction, that is, using whatever correction the subject has. This definition acknowledges the importance of uncorrected (or under-corrected) refractive error as a cause of vision loss worldwide and almost doubles the number of people counted as having vision loss.
In the United States and Canada, legal blindness is defined as best-corrected visual acuity equal to or less than 20/200 (6/60, 0.1), which corresponds with the ICD-8 criteria, or maximum diameter of visual field less than 20° in the better eye. Low vision has been defined as best-corrected visual acuity worse than 20/40 (6/12, 0.5) but better than 20/200 (6/60, 0.1). Across Europe the visual acuity criterion for registration as blind (or certification as severely sight impaired) varies, being less than 20/200 (6/60, 0.1) in the Republic of Ireland and Scotland, less than 20/400 (6/120, 0.05) in England, Wales, and Italy, and less than 20/1000 (6/300) in Germany. There is also a partially sighted (sight-impaired or significant visual impairment) category, for example in England and Wales being between 20/200 (6/60, 0.1) and 20/400 (6/120, 0.05) and in Scotland being worse than 20/60 (6/18, 0.33) but equal to or better than 20/200 (6/60, 0.1).
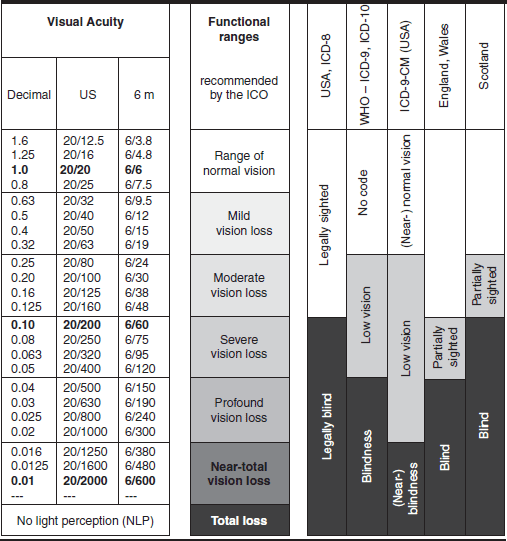
Table 20–1 shows the comparison between the ICD-8, ICD-9, ICD-9-CM, and ICD-10 major categories, the recommendations of the ICO and, as examples of variations within Europe, the criteria for registration in England, Wales, and Scotland. The differences emphasize the importance of knowing which definition was used whenever statistics about vision loss are compared. It should be noted that the ICO’s category of “Profound Vision Loss” is classified as blindness in ICD-9 but as (profound) low vision in ICD-9-CM to indicate that there still is useful residual vision.
In the United States the visual requirements for driving vary from state to state for both private and commercial drivers. 20/40 best-corrected visual acuity with both eyes is the most common requirement for private drivers, but some accept less. These requirements set a safety margin between letter chart performance in the office and on-the-road performance under adverse conditions. The requirements for commercial drivers are often more stringent, not because they drive in a different visual environment, but because a wider safety margin is deemed desirable. In Canada, the legal limit for driving for private drivers is best-corrected visual acuity with both eyes 20/50 (6/15) or better and a continuous field of vision horizontally no less than 120° and vertically 15° above and below central fixation, and with no evidence of diplopia within the central 40° of fixation. Responsible health professionals are legally obligated to report patients failing these requirements to the Ministry of Transportation. There are published vision standards for pilots and for admission to service academies.
Historically, prevalence studies on blindness were varied and inconsistent, making it difficult to compare reports from different parts of the world. Comparable data has become available from nearly every WHO member state allowing attempts at more accurate comparison of worldwide statistics. In a 2004 WHO report summarizing available population-based studies, the worldwide prevalence of profound vision loss (WHO blindness) was estimated to be 0.57%, and the worldwide prevalence of moderate low vision (WHO low vision) was estimated to be 2%. The prevalence of profound vision loss ranged from 0.2%–0.3% in developed countries in American, European, and the Western Pacific regions, to 1% in developing countries in the regions of Southeast Asia, the Eastern Mediterranean, and Africa. Prevalence of low vision largely followed these regional trends.
Approximately 314 million people worldwide are visually impaired from various causes (including uncorrected refractive error), 65 million of whom have profound vision loss. Population-based studies indicate that the global prevalence of vision loss has been declining since the early 1990s, with less vision loss from infectious diseases such as trachoma but increasing vision loss from conditions related to aging, such as cataract and age-related macular degeneration. Accordingly, the majority of the visually impaired are older (82% over the age of 50) but also poor, with close to 90% of the world’s visually impaired living in low and middle-income countries. Vision loss is additionally clustered into disadvantaged communities in rural areas and urban slums, where the risk of profound vision loss is 10–40 times higher than in the industrially developed regions of Europe and America. Women are at much higher risk of vision loss, population-based surveys estimating that 64% of those with vision loss worldwide are women. There are approximately 1.5 million children with profound vision loss in the world, with an annual incidence of 500,000 and 40% of cases being due to causes that are considered avoidable.
Although the ICD-9 definition of visual impairment is based on best-corrected visual acuity, nearly 153 million people worldwide have impaired vision (<20/60 to 20/200 in the better eye) due to uncorrected refractive error. It is estimated that over 12 million children (between the ages of 5 and 15) with impaired vision could have normal vision with correction of refractive error alone.
Overall, the leading causes of profound vision loss in the world, in order of decreasing prevalence, are cataract, uncorrected refractive error, glaucoma, and age-related macular degeneration (Table 20–2). Other major causes include corneal scarring, diabetic retinopathy, and trauma, the last being the most common cause of monocular profound vision loss globally. Vision loss caused by infectious diseases is decreasing due to improvements in public health. Trachoma affects 40 million people today, compared to 360 million in 1985.
| Cause | Percentage of Total Worldwide Blindness |
|---|---|
| Cataract | 39.1 |
| Uncorrected refractive error | 18.2 |
| Glaucoma | 10.1 |
| Age-related macular degeneration | 7.1 |
| Corneal opacities | 4.2 |
| Diabetic retinopathy | 3.9 |
| Childhood blindness | 3.2 |
| Trachoma | 2.9 |
| Oncocerciasis | 0.7 |
| Other | 10.6 |
Across the world, the relative prevalence of the different causes of vision loss is influenced by the level of social development and local geography. In developing countries, cataract is the leading cause, with glaucoma, trachoma, leprosy, onchocerciasis, and xerophthalmia also being important. Corneal scarring is a significant cause of monocular vision loss in the developing world, accounting for 850,000 cases of corneal profound vision loss per year in India alone. In more developed countries, vision loss is to a great extent related to the aging process. Although cataract is still an important cause of vision loss, the leading causes of profound vision loss in North America and other developed countries are age-related macular degeneration, diabetic retinopathy, and glaucoma. Other causes are herpes simplex keratitis, retinal detachment, retinal vascular disorders, and inherited retinal degenerative disorders.
With regards to global vision loss in children, retinal diseases such as retinopathy of prematurity (ROP) account for 29%, corneal scarring, predominantly due to xerophthalmia, rubella, and infection, accounts for 21%, and congenital disorders (including cataract, glaucoma, and structural abnormalities of the globe) accounts for 14%. Differences again exist when comparing the relative causes in developed and developing countries. In developed countries, the major causes are ROP, cataract, hereditary disease of the retina, diseases of the central nervous system (including hypoxic injury to the visual pathway), congenital malformations of the globe (microphthalmos, anopthalmos, and optic nerve hypoplasia), and nystagmus. The major causes in developing countries are corneal scarring, trachoma, genetic diseases, and cataract.
Close to 40% of profound vision loss worldwide can be attributed to cataract. In many parts of the developing world, the facilities available for treating cataract are grossly inadequate, hardly sufficient to cope with new cases and completely inadequate for dealing with the backlog of existing cases, currently estimated to be 10 million.
It is not fully understood why the frequency of cataract varies so greatly in different geographic areas, although exposure to ultraviolet radiation and recurrent episodes of dehydration, often occurring in severe diarrheal diseases, are thought to be important. With decreasing mortality rates and changing demographics, age-related causes of vision loss, including cataract, are expected to continue to rise. Worldwide, approximately 17 million people are currently blind from cataract. By 2020, this number is expected to reach 40 million. Although no current medical treatments exist to delay the development of cataract, it is estimated that a 10-year delay in cataract formation would reduce the number of individuals requiring surgery by 45%. Until an effective treatment that can prevent or delay cataract formation is devised, it will remain a leading cause of vision loss and will become an increasingly important global public health concern.
When included in the global statistics, uncorrected refractive error accounts for over 18% of profound vision loss, with a much larger percentage of moderate and severe vision loss, affecting approximately 8 million people with 1 million in India alone. It is clearly avoidable and should be easy to correct, provision of corrective lenses being the most cost-effective means of addressing a massive global health problem. However, uncorrected refractive error remains a major cause of vision loss throughout the world, even in developed countries such as the United States but particularly in developing countries where limited access to eye care professionals, low prevalence of eye health-seeking behavior, and low affordability of corrective lenses remain major problems. In children, ineffective screening also contributes.
The incidence of vision loss due to glaucoma has decreased in recent years as a result of earlier detection, improved medical and surgical treatment, and a greater awareness and understanding of the disorder by the lay population. However, in many developing countries, glaucoma remains the second most common cause of vision loss after cataract. This is especially the case in West Africa, where untreated open-angle glaucoma is extremely common. In China and Southeast Asia, there appears to be a preponderance of narrow-angle glaucoma. Glaucoma now blinds 6 million individuals worldwide, and a simple easy method of detecting patients at risk still does not exist. Treatment is also a major problem because of the poor compliance of most patients for taking daily eye drops. A simple but safe surgical procedure may ultimately be the only solution for reducing the needless burden of vision loss from this disease. More research in this area is essential.
Trachoma causes bilateral keratoconjunctivitis, generally in childhood that leads in adulthood to corneal scarring, which, when severe, causes vision loss. About 40 million people have trachoma, most of them in Africa, the Middle East, and Asia. It can be treated with various antibiotics, including tetracyclines and erythromycin, but azithromycin is proving to be the drug of choice. The number of individuals with profound vision loss from trachoma has dropped from 6 million to 1.3 million, which is a tribute to current WHO-supervised treatment programs and the effectiveness of azithromycin. However, to eliminate the disease will depend on global implementation of WHO’s SAFE strategy (Surgery for trichiasis, Antibiotic treatment, Face washing, and Environmental changes such as latrine building). Prevention of spread of infection will require provision of proper sanitary facilities, including clean water for drinking and washing, waste disposal, fly control, and behavioral change in hygiene.
Onchocerciasis is transmitted by bites of the blackfly, which breeds in clear running streams (hence the name river blindness). It is endemic in the greater part of tropical Africa and Central and South America. The most heavily infested zone is the Volta River basin, which extends over parts of Dahomey, Ghana, Ivory Coast, Mali, Niger, Togo, and Upper Volta. Worldwide, 15–20 million people are affected by onchocerciasis, with 20% of individuals in hyperendemic areas blinded by the disease.
The major ophthalmic manifestations of onchocerciasis are keratitis, uveitis, retinochoroiditis, and optic atrophy. The disease is prevented by insect eradication and personal protection by screening. Treatment with ivermectin is extremely effective in killing the microfilaria and sterilizing the adult females residing in nodules in the body. The effect of the mass distribution of ivermectin in areas where onchocerciasis is endemic is a public health success story. Like leprosy, onchocerciasis is definitely decreasing in its importance as a worldwide cause of vision loss because of successful treatment programs.
Age-related macular degeneration, diabetic retinopathy, and corneal disorders are discussed elsewhere in this and other chapters (see Chapters 6, 10, and 15).
Leprosy (Hansen’s disease) affects 14 million people in the world and has a higher percentage of ocular involvement than any other systemic disease. Up to 10% of leprosy patients are blind or visually impaired from the disease. The social stigma attached to leprosy has greatly hindered its treatment, but there are now highly effective chemotherapeutic agents that in most cases eradicate the infection. Effective treatment programs using triple drug therapy (dapsone, clofazamine, and rifampin) have markedly reduced the number of cases of leprosy worldwide as well as prevented the deformity and morbidity associated with the disease.
Xerophthalmia, due to hypovitaminosis A, is estimated to affect 5 million children each year. 500,000 develop corneal involvement, half of whom develop profound vision loss. It is a common cause of vision loss in infants, particularly in India, Bangladesh, Indonesia, and the Philippines. Clinically, there is xerosis of the conjunctiva with characteristic Bitot’s spots and softening of the cornea (keratomalacia), which may lead to corneal perforation. Protein malnutrition exacerbates the condition and renders it refractory to treatment. Affected infants often do not reach adulthood, dying from malnutrition, pneumonia, or diarrhea. Xerophthalmia can be prevented by general dietary improvement or vitamin A supplementation. If the problems of distribution and administration were solved, the cost of a quantity of the vitamin sufficient to prevent vision loss in 1000 infants would be only about $25. Measles immunization is also important because of the close association of measles epidemics with the blinding complications of xerophthalmia.
Hereditary conditions are important causes of vision loss but should gradually decrease in incidence in response to the efforts of genetic counselors to increase public awareness of the preventable nature of these disorders.
Prevention of Vision Loss
Preventive medicine is increasingly important in attempts to fulfill society’s expectations of modern medicine with the resources available. Although prevention is a logical approach to the solution of many problems in all branches of medicine, in practice there are a number of hurdles to be overcome. For any particular condition, it is essential that individuals at risk be easily identified. If their identification requires population screening, the screening process should be easy to perform, accurate, and reliable. Preventive measures must be both effective and acceptable to the target population. Unwarranted interference with the at-risk individual’s lifestyle only leads to poor compliance. Legislation may be required for certain measures but may engender resentment when it is felt to infringe on personal liberty. For preventive medicine to be successful, there must be cooperation among all segments of society—not just the medical community—in identifying problem areas, establishing workable solutions, and disseminating information. The successes that have been achieved in occupational health are an example of what can be accomplished if a consensus of opinion is established.
In ophthalmology, the major avenues for preventive medicine are ocular injuries and infections, genetic and systemic diseases with ocular involvement, and ocular diseases in which the early treatable stages are often unrecognized or ignored.
Ocular injuries are a very preventable cause of vision loss because simple preventive measures are often available. Injuries can vary from closed globe, such as blunt trauma or chemical injuries, to open globe injuries including rupture, perforation, and penetration (see Chapter 19). WHO statistics show that over 55 million eye injuries occur each year. 1.6 million people are rendered blind, 2.3 million develop bilateral low vision and 19 million have monocular blindness or low vision. The United States Eye Injury Register (USEIR) statistics show that over 57% of the injuries occur in people under 30 years of age, the percentage being even higher in work-related injuries.
Approximately 30% of all eye patients presenting to emergency departments have ocular trauma. Eye injuries remain a significant risk to worker health, especially among individuals in jobs requiring intensive manual labor.
Many manufacturing processes pose a particular threat to the eye. Grinding or drilling commonly propels small fragments of metal into the environment at high velocity, and these missiles can easily lodge on the cornea or penetrate the globe through the cornea or sclera. Tools with sharp ends, such as screwdrivers, are also commonly involved in producing penetrating ocular injuries. Welding arcs produce ultraviolet radiation that may cause epithelial keratitis (“arc eye”). Industrial chemicals—particularly those containing high concentrations of alkali or acid—can rapidly produce severe ocular damage that is often bilateral and associated with a poor visual outcome.
New legislation, increased worker training, particularly targeting groups most at risk, provision of effective eye protection equipment, and development of a culture of safety in the workplace, have led to a decline in eye injuries. Workers must be properly trained in the use of tools, machinery, and chemicals. Safety guards must be fitted to all machinery, and safety goggles must be worn whenever the worker is doing hazardous work or is in the workplace area where such hazards exist. It is surprising how many workers assume that they are no longer at risk of injury when they are not themselves performing hazardous tasks even though they are in the vicinity of work being performed by others.
The growing interest in “do-it-yourself” projects in the home exposes many more individuals to the risks of ocular injury from machinery, tools, and chemicals. Education of the public to recognize and minimize such risks, which may not be obvious to the ordinary householder or hobbyist, is particularly important.
Early recognition and urgent expert ophthalmologic assessment of any injuries sustained is essential. In the case of chemical injuries, immediate copious lavage of the eyes with sterile water, saline if available, or tap water for at least 5 minutes is the most important method of limiting the damage incurred. Neglect of penetrating injuries or corneal foreign bodies markedly increases the potential for long-term morbidity. Obtaining an accurate history is crucial in identifying the possibility of a penetrating injury. This is particularly true when medical help is sought some time after the injury and the patient may not realize the importance of a seemingly minor episode of trauma. Any worker who presents with unexplained visual loss or intraocular inflammation must be carefully questioned about the possibility of recent ocular injuries and the possibility of an occult intraocular foreign body borne in mind.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


