Introduction
Prompt recognition and treatment of ophthalmic emergencies are crucial to prevention of unnecessary visual impairment. Although specific diagnosis may require specialist ophthalmic expertise, using simple guidelines non-ophthalmologists as well as ophthalmologists can identify patients requiring emergency or urgent evaluation. Intensity and duration of pain, rapidity of onset and severity of visual loss (primarily assessed by visual acuity, which should be measured for each eye in all patients presenting with ophthalmic emergencies), gross appearance of the globe, and abnormalities on ophthalmoscopy are particularly important parameters.
Excluding ocular and orbital trauma, which is covered in Chapter 19, this chapter reviews the common ophthalmic emergencies, for the most part grouped according to the predominant symptom. For each group, the section on triage highlight the features that are crucial during initial assessment by a non-ophthalmologist, for instance on presentation to an emergency department. The section on clinical assessment emphasizes what is important during ophthalmological evaluation. The management of the more common or important entities is then briefly discussed, principally to provide reference to discussion in other chapters.
Acute Red Eye
The majority of patients with acute red eye have a relatively benign condition, such as bacterial, viral, or allergic conjunctivitis, subconjunctival hemorrhage, or blepharitis, which poses little or no threat to vision. Conversely a few are at risk of rapid progression within a few hours or days to severe visual impairment, even blindness, such as from acute angle closure glaucoma, intraocular infection (endophthalmitis), bacterial, viral, amebic, or fungal corneal infection, acute uveitis, or scleritis.
Emergency or urgent ophthalmic evaluation should be arranged for any patient with acute red eye and a history within the past few weeks of intraocular surgery, which predisposes to endophthalmitis; contact lens wear, which predisposes to corneal infection (see Figure 6–3); recent or distant history of corneal transplantation because of the possibility of graft rejection; previous episodes of acute uveitis or scleritis; or systemic diseases predisposing to uveitis or scleritis, such as ankylosing spondylitis and rheumatoid arthritis. In acutely ill patients, particularly those with sepsis or requiring prolonged intravenous cannulation such as in intensive therapy units or for parenteral nutrition, an acute red eye may be due to bacterial or fungal endophthalmitis (see Figure 15–32). Ocular involvement in toxic epidermal necrolysis, Stevens-Johnson syndrome, or erythema multiforme requires urgent ophthalmic assessment.
Pain, rather than discomfort, should be regarded as inconsistent with conjunctivitis, episcleritis, or blepharitis. It is suggestive of keratitis, intraocular or scleral inflammation, or elevated intraocular pressure, with the likelihood of a serious cause increasing with increasing severity. Associated nausea and vomiting are particularly suggestive of markedly elevated intraocular pressure. Deep, boring pain, typically waking the patient at night, is characteristic of scleritis. Photophobia characteristically occurs in keratitis and anterior uveitis.
Reduced vision, whether reported by the patient or identified by measurement of visual acuity, in the absence of a pre-existing explanation, should also be regarded as inconsistent with conjunctivitis, episcleritis, or blepharitis and, as with pain, the greater the severity the greater the likelihood of a serious cause.
Severity of redness is not necessarily a guide to the seriousness of the underlying condition, for instance subconjunctival hemorrhage with its bright red appearance being a benign entity (see Figure 5–34). Distribution of redness can be helpful, with predominance around the limbus (circumcorneal) being indicative of intraocular disease, whereas diffuse redness involving the tarsal and bulbar conjunctiva being indicative of conjunctivitis (see Figure 16–1); focal or diffuse redness of the globe being consistent with episcleritis; and redness of the eyelid margins being indicative of blepharitis. Bluish redness (violaceous discoloration) of the globe (see Figure 7–28), best identified in natural rather than artificial light, is characteristic of scleritis. Vesicles or ulceration of the lids or periocular skin are typical of ophthalmic zoster (shingles) (see Figure 5–13) and less commonly varicella or primary herpes simplex virus infection.
Conjunctivitis usually causes purulent, mucoid, or watery discharge, and allergic conjunctivitis typically causes itching. Profuse purulent discharge is characteristic of gonococcal conjunctivitis, which requires emergency treatment (see later in the chapter).
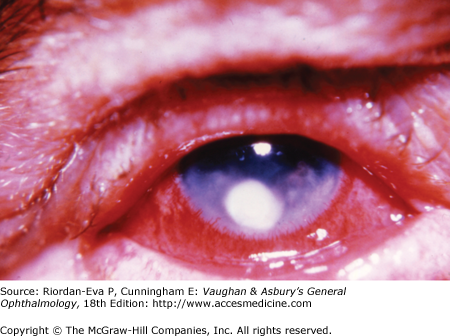
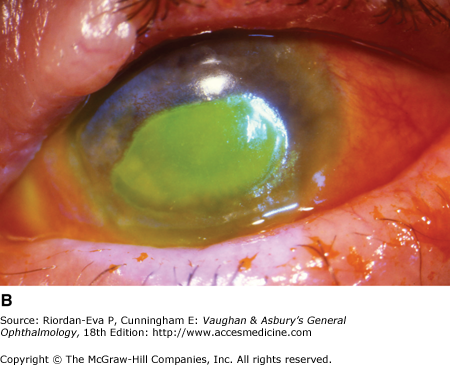
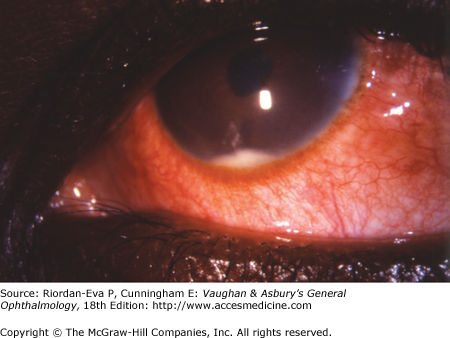
Any abnormality of the cornea apparent on gross examination, such as ulceration (Figure 3–1) or focal opacity (Figure 3–2), which may be due to infection, or diffuse cloudiness, which may be due to markedly elevated intraocular pressure when it is usually associated with a semi-dilated unreactive pupil, warrants emergency ophthalmic assessment unless it is known to be longstanding, for example pterygium (see Figure 5–32). Instillation of fluorescein facilitates identification of an epithelial defect (Figure 3–3), including dendritic ulceration due to herpes simplex virus keratitis (see Figure 5–10). A constricted pupil is suggestive of intraocular inflammation, typically due to anterior uveitis. Hypopyon (pus within the anterior chamber), a feature of corneal infection, intraocular infection, or acute anterior uveitis (iritis) (see Figures 3–4 and 16–5), necessitates emergency ophthalmic assessment.


Slitlamp examination (see Figure 2–6) facilitates assessment of distribution of redness; identification of conjunctival abnormalities, including examination of the superior tarsal conjunctiva following eversion of the upper eyelid (see Figure 2–7); diagnosis of episcleritis and scleritis (see Figures 7–26 to 7–29); characterization of corneal lesions; and detection of corneal keratic precipitates (see Figure 7–3), anterior chamber flare and cells, and possibly hypopyon indicative of anterior chamber inflammation due to anterior uveitis, intraocular infection, or secondary to corneal inflammation, including infection. In cases of intraocular inflammation, dilated fundal examination is essential to determine whether there is involvement of the vitreous, retina (see Figures 7–8, 15–30, 15–31 and 15–33) or choroid (see Figures 15–25 and 15–27), which is important to diagnosis as well as assessment of severity.
There are many causes of acute conjunctivitis (see Table 5–1), which in most case is a benign, often self-limiting, condition (see Chapter 5). However care needs to be exercised in neonates (ophthalmia neonatorum) (see Chapter 17) because of the possibility of infection with chlamydia, which may be associated with non-ocular disease and needs systemic therapy, gonococcus, or herpes simplex virus, which may be associated with encephalitis and requires hospitalization and parenteral antiviral therapy. Gonococcal conjunctivitis in neonates or adults, characteristically causing profuse purulent discharge (see Figure 5–1) as well as severe conjunctival inflammation, necessitates emergency investigation by microscopy and culture of the discharge and parenteral antibiotic therapy with ceftriaxone to avoid progression to severe corneal damage (see Table 6–1). Treatment with parenteral antiviral therapy within 72 hours of the appearance of the rash reduces the likelihood of ocular complications in ophthalmic zoster (shingles) (see Chapters 5 and 6). Skin lesions on the tip of the nose (Hutchinson’s sign) or the eyelid margins are predictive of ocular complications.
Management of acute keratitis primarily revolves around identification and treatment of infection, for which contact lens wear and pre-existing ocular surface disease, including corneal anesthesia or exposure, are the common predisposing factors (see Chapter 6). Occasionally it is apparent straightaway that there is a non-infectious inflammatory process, requiring other therapy, possibly topical or systemic steroids but steroid therapy should not be started without ophthalmic assessment.
Management of acute intraocular inflammation (uveitis) also primarily revolves around identification and treatment of infection, particularly if there is posterior segment involvement (vitritis, retinitis, or choroiditis) or recent history of intraocular surgery, but a non-infectious inflammatory process is more common than in acute keratitis. Topical or systemic steroid therapy should not be started without ophthalmic assessment. Scleritis is infrequently caused by infection, autoimmune disease being more commonly responsible (see Table 7–7), and can often be managed in the first instance by oral nonsteroidal anti-inflammatory agents (NSAIDS) but ophthalmic assessment is necessary to make the diagnosis and exclude other entities.
In acute angle closure glaucoma prompt recognition and treatment are required if severe visual loss is to be avoided (see Chapter 11). The mainstay of initial treatment is intravenous and oral acetazolamide, as well as topical agents, to reduce intraocular pressure, supplemented by topical steroids to reduce inflammation, and topical pilocarpine to constrict the pupil. Definitive treatment is usually laser peripheral iridotomy with prophylactic treatment to the fellow eye. Emergency ophthalmic assessment is essential to establish the diagnosis, including exclusion of other causes of markedly raised intraocular pressure that may require distinctly different treatment.
Acute Orbital Disease
Acute orbital disease is uncommon but a few entities need to be recognized promptly to avoid the severe visual loss, or even non-ocular morbidity and possibly mortality that may result from delay in treatment (see Chapter 13).
Orbital cellulitis is usually a disease of childhood and due to spread of infection from the ethmoid sinuses. It is characterized by fever, pain, eyelid swelling and erythema, proptosis, limitation of extraocular movements, and systemic upset with leukocytosis. Pre-septal cellulitis, in which there is no proptosis or limitation of eye movement, may be due to a localized infection in the anterior (pre-septal) portion of the eyelid or may be the early manifestation of orbital cellulitis. In adolescents and young adults orbital signs may be indicative of extension of infection from the fronto-ethmoidal sinus complex. In diabetics and the immunocompromised, acute orbital disease may be due to fungal infection (mucormycosis), with a high risk of death even with early treatment.
Usually occurring in patients with autoimmune hyperthyroidism (Grave’s disease), which may or may not have been diagnosed previously, acute Graves’ ophthalmopathy may lead to marked proptosis (see Figures 5–30, 13–3 and 15–23), with the possibility of corneal exposure or optic nerve compression, and limitation of eye movements. Pseudotumor, another inflammatory orbital disease, and carotid artery-cavernous sinus fistula, due to dural shunts that typically occur in patients with diabetes and/or systemic hypertension, or due to spontaneous rupture of an intracavernous internal carotid artery aneurysm, may present in a similar manner.
Reduced vision unexplained by corneal exposure, especially if associated with impaired color vision and/or a relative afferent pupillary defect, indicates optic nerve dysfunction. In orbital cellulitis non-axial proptosis implies abscess formation. Other complications include cavernous sinus thrombosis and intracranial infection, the latter being more likely if there is infection in the frontal sinus.
Orbital cellulitis is a clinical diagnosis and requires hospitalization and immediate institution of antibiotic therapy, usually intravenously, together with early ophthalmic and otolaryngologic assessments. Orbital imaging may be undertaken in all cases or reserved for those in whom orbital abscess or another complication is suspected.
Orbital imaging, usually CT but possibly MRI, is generally sufficient to differentiate between Graves’ ophthalmopathy, orbital pseudotumor, and carotid artery-cavernous sinus fistula, but orbital ultrasound blood flow studies are particularly helpful in diagnosing the third.
Acute Painless Visual Loss
Sudden onset painless visual loss is a very important symptom, because it may be due to ophthalmic disease that requires emergency or urgent treatment; ocular vascular disease with immediate or early threat to the patient’s life or remaining vision; or acute intracranial disease.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


