Chapter 61 Vision, reading and dyslexia
Reading
In an alphabetic language (such as English), poor phonological skills compromise the development of grapheme-phoneme mappings. This is the cornerstone of the current understanding of the term dyslexia.1,2
Dyslexia
A definition of the term dyslexia is emerging. This is due to be published in DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, American Psychiatric Association), and is outlined in Box 61.1.3
Box 61.1 Proposed definition of dyslexia
DSM-5
A. Difficulties in accuracy or fluency of reading that are not consistent with the person’s chronological age, educational opportunities, or intellectual abilities
B. The disturbance in criterion A, without accommodations, significantly interferes with academic achievement or activities of daily living that require these reading skills
The major change (from the 1994 definition) is the removal of discrepancy between general cognitive ability and reading skills. While a discrepancy between achievement (in reading) and intellectual ability may still be present, it is now appreciated that all dyslexic children, irrespective of intellectual ability, have the same poor phonological skills.2 Furthermore, all groups demonstrate similar improvement as a result of evidence-based phonological interventions.4,5
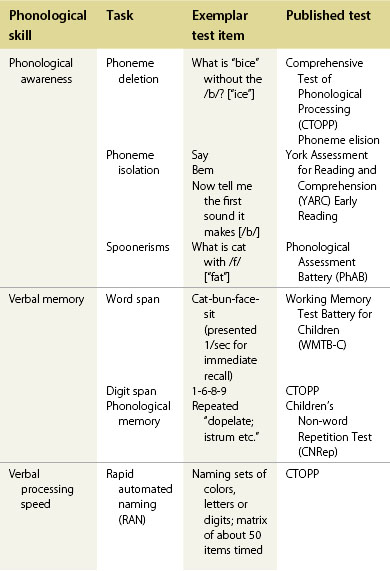
An independent report, authored by Sir Jim Rose, formerly Her Majesty’s Inspector and Director of Inspection for the Office for Standards in Education (Ofsted), defined dyslexia as outlined in Box 61.2.6 Point 2 illustrates the three areas of phonological processing initially described by Wagner and Torgeson:7
a. Phonological awareness: the ability to attend to and manipulate sounds in words.
b. Phonological memory: memory for speech-based information – sometimes called verbal memory.
c. Naming (providing the spoken label for visual referent) or verbal processing speed.
Box 61.2 Definition of dyslexia
Rose Report on Dyslexia 2009
1. Dyslexia is a learning difficulty that primarily affects the skills involved in accurate and fluent word reading and spelling
2. Characteristic features of dyslexia are difficulties in phonological awareness, verbal memory, and verbal processing speed
3. Dyslexia occurs across the range of intellectual abilities
4. It is best thought of as a continuum, not a distinct category, and there are no clear cut-off points
5. Co-occurring difficulties may be seen in aspects of language, motor co-ordination, mental calculation, concentration, and personal organization, but these are not, by themselves, markers of dyslexia
6. A good indication of the severity and persistence of dyslexic difficulties can be gained by examining how the individual responds or has responded to well-founded intervention
Dyslexia is common (5% of the population).8 It is distributed equally between the sexes,9,10 is familial, and persistent.
Dyslexia was originally a behavioral description (inaccurate or dysfluent word reading or spelling), but is now based on a defect at a cognitive level (poor phonological processing).8 Functional MRI findings demonstrate (in adults) activity in the left parietotemporal region during word analysis involving phonemes, and the left occipital temporal region for automatic rapid responding. The latter predominates in skilled reading.8 There is evidence that children with dyslexia rely on other areas (such as the inferior frontal gyrus and other right hemisphere sites) during reading, possibly as a result of compensatory processes. Anterior cortical areas, involved in articulation, may contribute in developing phoneme awareness (forming the words with the lips and tongue).
Reading assessment
Phonological processes are examined in a variety of ways (Table 61.1). Most of these tests have been validated in children of different ages.
Dyslexia management
Prospective studies show that 8-year-old dyslexics demonstrated weak letter knowledge in reception classes at school (age 4−5 years) and poor phoneme awareness in year 1.11,12 It is desirable to identify these children early and to supply early support before these children fail.4,13
There are many publications (see Snowling4) demonstrating reading improvement using phonological based packages. Delay in applying these can lead to harm. Children who fail become disruptive, avoid reading, and cannot access academic material.
The visual system
A working visual system is required to see the script. The areas available to examine and manipulate are up-stream from the pathology of dyslexia, as outlined above. The eye care practitioner’s role is to exclude any visual problem. Elucidating whether any visual abnormality coexists and whether it is causative or secondary to poor reading may be difficult (see Handler14 and the AAO joint statement15).



