19
Vibratory Asymmetry
The evaluation of a patient with hoarseness begins with the clinician listening to the patient’s voice. As soon as the patient vocalizes, the clinician begins to gather clues about the source of the pathology. A raspy or rough voice suggests irregular or aperiodic vibration of the vocal folds. Even small changes in vocal fold vibration can result in large changes in vocal quality.15 To determine if vibratory abnormalities are the source of vocal changes, an evaluation of vocal fold vibration with videostroboscopy is required.
Symmetry of vocal fold vibration is defined as the degree to which the vocal folds are mirror images of one another during vibration. Asymmetry of vibration can occur due to asymmetry in the timing (phase) or amplitude of the mucosal wave (Fig. 19.1).6 Although asymmetry, particularly phase asymmetry, is not specific and does not always signify pathology, asymmetry of vocal fold vibration usually suggests a difference in the viscoelastic or mechanical properties of the vocal folds. This includes differences in mass, shape, position, tension, and elasticity.6–8 Often more than one property is affected. Very commonly, asymmetry of vibration is the result of a decrease in the amplitude of vibration of one of the vocal folds relative to the other due to unilateral vocal fold pathology (Video Clips 32 to 34).
Sometimes the reason for vibratory asymmetry is obvious, such as a large mass on one vocal fold, or it may be subtle, as in the case of unilateral submucosal fibrosis. If one vocal fold vibrates normally and the other one does not, asymmetry should be easy to identify. When pathology involves both vocal folds, asymmetry may be more difficult to recognize, but doing so will help the clinician to make appropriate treatment decisions. For example, a patient with unilateral Reinke’s polyposis and a poorly vibrating contralateral vocal fold should be treated more conservatively than a patient with a normal contralateral vocal fold. Overaggressive resection of the polyp or poor healing at the site of resection could result in scar, which, along with an abnormal contralateral vocal fold, would require high phonation pressures to vocalize and result in a very rough, strained voice. It might be more prudent to avoid surgery in such cases or perform a very conservative excision. In addition, asymmetry of vibration in patients with bilateral Reinke’s polyposis may suggest unilateral sulcus or scar that should also lead to caution on the part of the surgeon (Fig. 19.2).
 Coupling
Coupling
Vocal folds with different viscoelastic properties can still appear to vibrate synchronously through a process called coupling. Because of the coupling effect, subtle asymmetry may not be detected either in vocal quality or on videostroboscopic examination. More severe viscoelastic asymmetry and asymmetry in vocal fold position can compromise coupling and yield only partial synchronization of vibration resulting in bifurcations or modulations (Video Clip 23). Clinically, this may manifest as diplophonia or the perception of two or more simultaneous pitches in the patient’s voice. Diplophonia occurs through quasi-periodic variations in vocal fold vibration. The acoustic structure of diplophonia can be appreciated with narrow-band spectrography. Spectrography demonstrates subharmonics and perturbation within vibratory cycles (Fig. 19.3). Subglottic pressure and airflow contribute to the efficiency of coupling and can mask vocal fold asymmetry.7,9–11 It is important, therefore, to have the patient phonate at different volumes and pitches during the videostroboscopic examination to illicit subtle asymmetry in vibration (Video Clips 38 and 39).
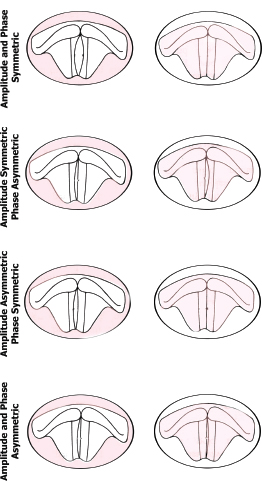
Fig. 19.1 Phase and amplitude asymmetry.
 Interpretation of Vibratory Asymmetry
Interpretation of Vibratory Asymmetry
When asymmetric vibration is observed during videostroboscopy, the examiner needs to consider the differences in the mechanical properties of each vocal fold that are likely contributing to the asymmetry. A unilateral decrease in vibratory amplitude will result in asymmetric vocal fold vibration. As a result, when considering the differential diagnosis of asymmetric vocal fold vibration, there is significant overlap with the differential diagnosis of decreased vibratory amplitude.
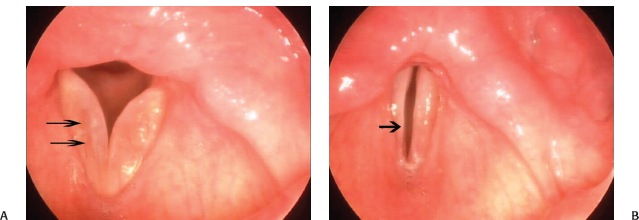
Fig. 19.2 (A) Bilateral Reinke’s polyposis in a patient who presented 15 years after having a unilateral polypectomy. The right vocal fold has a sulcus superior to the remaining Reinke’s polyposis. The mucosal wave was impaired on the right. Extra care must be taken to avoid sulcus on the contralateral side or the patient might be left with a worse voice. In fact, the surgeon may operate on only the right vocal fold polyp and wait to decide if contralateral surgery is necessary after allowing the patient to heal. Double arrows point to a sulcus superior to the remaining Reinke’s polyposis on the right vocal fold. (B) Scarring of the right vocal fold is more apparent during phonation.
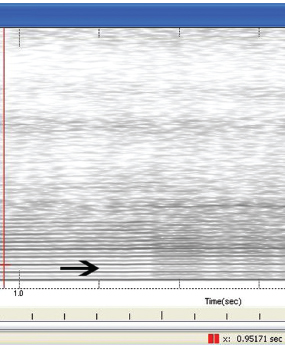
Fig. 19.3 Spectrogram: Narrow-band sustained vowel /a/ with subharmonics. The arrow points to subharmonics.
Vocal Fold Masses
Although, in general, an increase in the mass of the vocal fold will result in a reduction of the vocal fold vibration amplitude (and, in cases of a unilateral change in mass, result in vibration asymmetry), distinct vocal fold masses affect vibration differently. Zhang and Jiang developed a unilateral vocal fold polyp model and demonstrated that the larger the polyp, the larger the degree of vocal fold vibration asymmetry. In addition, the larger the polyp, the greater its nonlinear effect on vocal fold vibration and the more likely it is for chaotic vibration to occur.4,12 Although it seems logical that the size of a vocal fold mass will contribute to the degree of asymmetry, other properties of the mass, such as firmness, shape, and depth, will also have ramifications on vocal fold vibration. It is difficult to define the effects of a mass on vocal fold vibration based on its etiology and nomenclature alone.
Small unilateral superficial lesions such as vocal fold polyps, papilloma, and noninvasive leukoplakia may not have a dramatic affect on the amplitude of horizontal vocal fold excursion. It is the localized effect of the lesion on the stiffness of the vocal fold cover that determines the impact of the lesion on vibration at that location. This will depend on how firm or fibrotic the lesion is or if there is surrounding submucosal fibrosis or invasion. A long-standing vocal fold polyp may become firm and fibrotic or develop significant fibrosis at the base, which will result in a localized hypodynamic segment (Video Clip 19). This is important to note, to appropriately counsel patients and temper expectations, if surgical intervention is necessary. Leukoplakia and papilloma tend to increase the stiffness of the cover and result in decreased vibration. However, significantly reduced vibration in the presence of leukoplakia must raise suspicion for an invasive process, such as carcinoma (Video Clip 35). Of course, the degree of invasion can be assessed at the time of surgery with palpation and hydrodissection, but preoperative recognition is important for patient counseling and preparation. The surgeon can prepare the patient for the possible necessity of a wider excision than might be required for dysplasia or hyperkeratosis, involving more than only the superficial epithelium.
If superficial bilateral masses exist, asymmetry of vibration will be determined by the different morphologic characteristics of the masses and how the masses interact. For example, true vocal fold nodules are symmetric and will likely affect the vibratory characteristics of each respective vocal fold to the same degree, so that vibration will remain symmetric (Video Clips 18 and 40). A soft, small hemorrhagic polyp and a firm fibrotic contact mass, however, will likely result in asymmetric vibration. If the lesions interfere with each other, vibration will be chaotic bilaterally.6
Lesions that extend deeper into the vocal fold tend to affect vibration more significantly then superficial lesions. Reinke’s polyposis involves the entire superficial layer of the lamina propria, increasing the mass of the vocal fold and resulting in reduced vibratory amplitude. The consistency of the Reinke’s stroma will determine how vibration is affected. If the stroma is more fluid, vibration amplitude may not be compromised and may even appear to be increased. If the stroma is more dense and fibrotic, the amplitude of vibration will be reduced or chaotic. As mentioned, a sulcus within Reinke’s polyposis will also affect vibration (Fig. 19.2). Submucosal cysts usually result in a more dramatic effect on vibration than do superficial lesions. Amplitude and mucosal wave are decreased and vibration is impaired at the site of the cyst (Video Clips 26 and 34). In general, deeper cysts, particularly if they abut the vocal ligament, will severely impair vibration (Fig. 19.4). Invasive malignancies will reduce vibration, increasing mass and stiffness of the vocal fold. As they invade the vocal ligament and vocalis muscle, vibration becomes severely compromised, and vibratory asymmetry becomes more pronounced (Video Clip 35).
As any asymmetry in the mass of the vocal folds results in vibratory asymmetry, a unilateral decrease in mass (as opposed to an increase in mass as a result of vocal fold pathology) may also present with vibratory asymmetry. This situation might occur after recovery from vocal fold paralysis or persistent paresis (Video Clips 41 and 42).
Vocal Fold Stiffness
Scar and Sulcus Vocalis
A difference in the stiffness of the superficial tissues of one vocal fold relative to the other will result in vibratory asymmetry. Stiffer tissues are not displaced as much as normal tissues during vibration. A unilateral or localized reduction in vibratory amplitude and mucosal wave, in the absence of a discreet mass, is often a result of increased tissue stiffness due to scar or a sulcus vocalis lesion. The injury may be localized, such as in the site of a previous surgical excision, or involve the entire length of the vocal fold. In general, location and depth of the lesion will determine its effect on vibration and voice. Deep scars and scars involving the mid-membranous portion of the vocal fold will be more symptomatic than superficial scarring or scars in the posterior third of the vocal fold (Video Clips 32, 33, and 43). Furthermore, voice manifestations will be less severe in the setting of unilateral stiffness involving the entire vocal fold. If the contralateral vocal fold is pliable and glottic closure is good, voice is usually not as severely affected as it would be in the case of bilateral vocal fold scar.
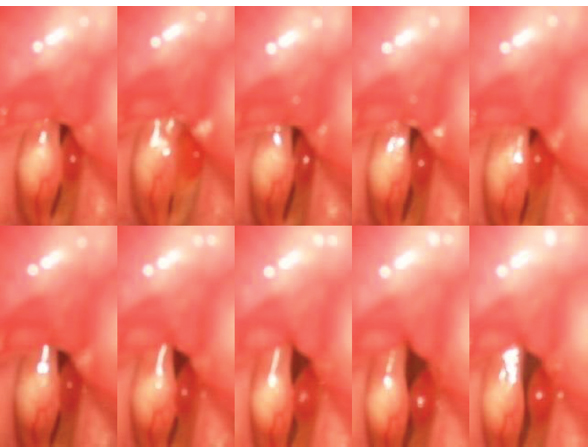
Fig. 19.4 Montage of vibratory cycle in a patient with a large right submucosal cyst and a soft, left hemorrhagic polyp. The amplitude of vibration is more compromised on the side with the cyst as it involves the deeper layers of the vocal fold.
The terms scar and sulcus are often used interchangeably. Both contribute to irregular or decreased vibration secondary to a loss of pliability and bulk of the vocal fold cover. In general, sulcus refers to a groove within the medial edge of the vocal fold. The etiology is unknown, but there appears to be migration of epithelium into the lamina propria. Scar results from replacement of normal superficial lamina propria with disorganized collagen fibers. The voice impact of both entities results from irregularity in vibration and glottic insufficiency.13–16
Ford et al. described three types of sulcus. Type I, or “physiologic sulcus,” is a depression along the entire length of the vocal fold, resulting from migration of the epithelium into the superficial lamina propria, but not all the way to the vocal ligament. Type II also involves the entire length of the vocal fold, but the epithelium migrates to the vocal ligament or deeper. Type III is a localized deep “pit.”4 It may easily be missed on videostroboscopy.15,16
On videostroboscopic evaluation, scar or sulcus may result in decreased or aperiodic vocal fold vibration, a concavity or groove along the medial edge, “spindle-shaped” glottis, a whitish-hue to the vocal fold, and a thickened appearance to the cover of the vocal fold. Again, findings will depend on the severity and size of the lesion. A small sulcus or scar will result in a localized hypodynamic segment, and more diffuse scarring will result in a generalized reduction in the mucosal wave (Fig. 19.5). Asymmetry may become more apparent at different pitches. Localized hypodynamic segments often present more clearly at higher pitches when the vocal fold is stretched, resulting in a stiffer cover.
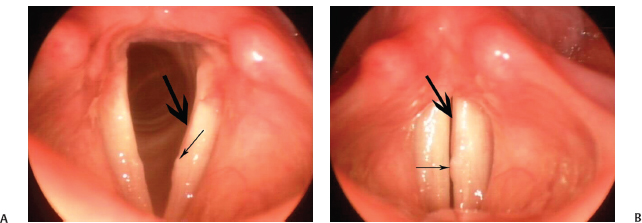
Fig. 19.5 (A) A 40-year-old woman who presented 5 months after having a left Reinke’s polyp removed by another surgeon. She was still dysphonic. The surgeon told her she had a recurrent mass on her left vocal fold that needed excision (thin arrow). She presented for a second opinion. Videostroboscopy showed asymmetric vibration with a severely reduced amplitude of vibration of the left vocal fold. The vocal fold was severely hypodynamic along the entire medial edge due to scarring along the entire length of the vocal fold (thickarrow). The patient was advised in our clinic that the scarring was the main reason for her dysphonia. (B) Patient during vocal fold adduction.
Acute Phonotrauma
Vocal fold tears and vocal fold hemorrhages result from acute phonotrauma. Vocal fold tears are subtle mucosal disruptions, typically at the mid-membranous portion of the vocal fold. On videostroboscopy, they are often unilateral and present as a hypodynamic segment. A linear disruption in the mucosa can often be visualized when the videostroboscopy recording is played back frame by frame. At other times, a focal area of inflammation around the tear is appreciated.17,18
Vocal fold hemorrhages occur because of a ruptured blood vessel. When superficial, they may have little-to-no effect on vocal fold vibration. However, deeper hemorrhages increase both the mass and stiffness of the vocal fold resulting in decreased amplitude of vibration and mucosal wave (Video Clip 44). Identifying and treating hemorrhages and tears appropriately is important to avoid long-term vocal fold scarring and mass formation.17,18
Vocal Fold Tension
Superior Laryngeal Nerve Paralysis
Asymmetry in the tension of each vocal fold often manifests as asymmetry in both the phase and amplitude of vibration during phonation.8 Vocal fold tension is primarily the result of contraction of the vocalis muscle and the viscoelastic properties of the vocal ligament. It contributes to medial compressive forces needed to create resistance to air flow through the glottis.19
Secondarily, an increase in vocal fold tension occurs as a result of cricothyroid muscle contraction. Contraction of the cricothyroid muscle alters the angle between the thyroid and cricoid cartilages, increasing the distance between the vocal processes of the arytenoid cartilages and the anterior commissure of the thyroid cartilage. This process elongates the vocal fold, thus increasing vocal fold tension, vibratory frequency, and vocal pitch. The cricothyroid muscle is innervated by the external branch of the superior laryngeal nerve. If this nerve is injured, the vocal fold of the affected side will be lax at higher pitches relative to the unaffected side (Fig. 19.6). Increased vocal fold laxity results in an increased vibratory amplitude and more chaotic vibration during phonation. The lax vocal fold is more sensitive to changes in subglottic pressure and airflow, which increases voice perturbation.1,7–9,2021

Fig. 19.6 Rigid videostroboscopy of a patient with right superior laryngeal nerve paresis. Right vocal fold is flaccid with increased vibration amplitude. The posterior larynx tilts to the right.
Superior laryngeal nerve paresis or paralysis can be difficult to diagnose by videostroboscopic examination. Phase and amplitude asymmetry, though they may be the only findings in superior laryngeal nerve palsy, are not specific to the diagnosis. Other findings that may occur, and therefore help to confirm the diagnosis, include vocal fold lag, posterior glottic tilt, and vocal fold height discrepancy.7,20,21
Recurrent Laryngeal Nerve Injury
Injury to the recurrent laryngeal nerve will result in denervation of the thyroarytenoid muscle. A flaccid paralysis results and the vocal fold appears bowed. However, spontaneous reinnervation is common after recurrent laryngeal nerve injury. Because of synkinesis, vocal fold movement may not be restored in cases of reinnervation, but tone will improve, and vibratory asymmetry may not be as prominent. If vocal fold paresis or paralysis occurs because of an upper motor neuron injury, vocal fold tone may be paradoxically increased or “spastic.” Increased tone results in a decreased amplitude of vibration, whereas decreased tone results in an increased amplitude of vibration (Fig. 19.7).20,21
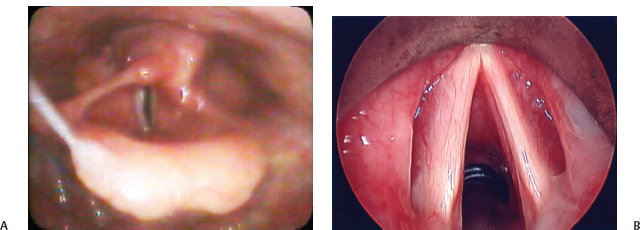
Fig. 19.7 (A) Flexible (distal chip) videostroboscopy demonstrating flaccid right vocal fold in a patient with a RLN paralysis. (B) Operative view prior to injection laryngoplasty. Note the severe atrophy of the right vocal fold.
The vibratory effect from a unilateral vocal fold paralysis is largely determined by the degree of glottic insufficiency, in other words, the size of the glottic gap. Vocal fold coupling is less efficient with a large glottic gap, resulting in more chaotic vibration. Increased airflow can compensate for glottic insufficiency, but this too becomes less effective as the gap widens (Video Clips 25, 27, and 28). Additionally, asymmetry in vocal fold height (another feature that may be seen with unilateral vocal fold paralysis or paresis) can result in more chaotic vibration.1,8,11 Vocal fold height is best evaluated using a 70-degree rigid telescope during videostroboscopy.20,21 Recognizing height discrepancy is important, as it may need to be addressed in addition to improving glottic closure during laryngeal framework surgery.
 Conclusion
Conclusion
Evaluation of vibratory symmetry is an important aspect of a videostroboscopic examination. Asymmetric vibration may be the result of differences in the amplitude of horizontal vocal fold excursion or the timing of vocal fold excursion. Although not always pathologic, asymmetry suggests a difference in the mass, tension, or viscoelastic properties between the two vocal folds. When there is not an obvious mass, asymmetry in vocal fold vibration may be the only visible clue to the etiology of the voice problem. It may be suggestive of a submucosal process such as scar or muscle weakness.
References
1. Plant RL. Aerodynamics of the human larynx during vocal fold vibration. Laryngoscope 2005;115:2087–2100
2. Herzel H. Possible mechanisms of vocal instabilities. In: Davis P, Fletcher N, eds. Vocal Fold Physiology: Voice Quality Control Controlling Complexity and Chaos. San Diego, CA: Singular Publishing Group; 1996:63–75
3. Titze IR, Baken RJ, Herzrl H. Evidence of chaos in vocal fold vibration. In: Titze IR, ed. Vocal Fold Physiology: Frontiers in Basic Science. San Diego, CA: Singular Publishing Group; 1993:143–182
4. Jiang JJ, Zhang Y, McGilligan C. Chaos in voice, from modeling to measurement. J Voice 2006;20:2–17
5. Berry DA, Herzel H, Titze IR, Krischer K. Interpretation of biomechanical simulations of normal and chaotic vocal fold oscillations with empirical eigenfunctions. J Acoust Soc Am 1994;95:3595–3604
6. Hirano M, Bless DM. Videostroboscopic Examination of the Larynx. San Diego, CA: Singular Publishing Group; 1993
7. Maunsell R, Ouaknine M, Giovanni A, Crespo A. Vibratory pattern of vocal folds under tension asymmetry. Otolaryngol Head Neck Surg 2006;135:438–444
8. Isshiki N, Tanabe M, Ishizaka K, Broad D. Clinical significance of asymmetrical vocal cord tension. Ann Otol Rhinol Laryngol 1977;86(1 Pt 1):58–66
9. Giovanni A, Ouaknine M, Guelfucci R, Yu T, Zanaret M, Triglia JM. Nonlinear behavior of vocal fold vibration: the role of coupling between the vocal folds. J Voice 1999;13:465–476
10. Berry DA, Herzel H, Titze IR, Story BH. Bifurcations in excised larynx experiments. J Voice 1996;10:129–138
11. Hong KH, Kim HK. Diplophonia in unilateral vocal fold paralysis and intracordal cyst. Otolaryngol Head Neck Surg 1999;121:815–819
12. Zhang Y, Jiang JJ. Chaotic vibrations of a vocal fold model with a unilateral polyp. J Acoust Soc Am 2004;115:1266–1269
13. Pontes P, Behlau M. Treatment of sulcus vocalis: auditory perceptual and acoustical analysis of the slicing mucosa surgical technique. J Voice 1993;7:365–376
14. Bouchayer M, Cornut G, Witzig E, Loire R, Roch JB, Bastian RW. Epidermoid cysts, sulci, and mucosal bridges of the true vocal cord: a report of 157 cases. Laryngoscope 1985;95(9 Pt 1):1087–1094
15. Dailey SH, Ford CN. Surgical management of sulcus vocalis and vocal fold scarring. Otolaryngol Clin North Am 2006;39:23–42
16. Ford CN, Inagi K, Khidr A, Bless DM, Gilchrist KW. Sulcus vocalis: a rational analytical approach to diagnosis and management. Ann Otol Rhinol Laryngol 1996;105:189–200
17. Klein AM, Johns MM III. Vocal emergencies. Otolaryngol Clin North Am 2007;40:1063–1080, vii
18. Sataloff RT, Spiegel JR, Hawkshaw M. Acute mucosal tear and vocal fold hemorrhage. Ear Nose Throat J 1994;73:633
19. Titze IR. Control of fundamental frequency. In: Titze IR, ed. Principles of Voice Production. Englewood Cliffs, NJ: Prentice-Hall; 1994
20. Rubin AD, Sataloff RT. Vocal fold paresis and paralysis. In: Sataloff RT, ed. Professional Voice: The Science and Art of Clinical Care, 3rd ed. San Diego, CA: Plural Publishing; 2005
21. Rubin AD. Neurolaryngologic evaluation of the performer. Otolaryngol Clin North Am 2007;40:971–989
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


