Essentials of Diagnosis
General Considerations
Vestibular schwannomas (VS) (acoustic neuromas) are nerve sheath tumors of the superior and inferior vestibular nerves (cranial nerve VIII). They arise in the medial internal auditory canal (IAC) or lateral cerebellopontine angle (CPA) and cause clinical symptoms by displacing, distorting, or compressing adjacent structures in the CPA.
VS are by far the most common tumors involving the CPA. VS make up 80% of CPA tumors and 8% of all intracranial tumors. Various epidemiology studies have shown an incidence of 10 per 1 million individuals each year. This figure correlates with 2000–3000 individuals diagnosed with VS each year in the United States. There is no gender bias and the age of presentation is between 40 and 60 y of age. Ninety-five percent of VS occur in a sporadic fashion. The remaining 5% of patients have neurofibromatosis type 2 (NF2) or familial VS. The age of presentation is earlier in nonsporadic VS and patients usually present in the second or third decades of life.
Anatomy
The CPA consists of a potential cerebrospinal fluid (CSF)-filled space in the posterior cranial fossa bounded by the temporal bone, cerebellum, and brainstem. The CPA is a roughly triangular-shaped structure in the axial plane and is filled with CSF (Figure 61–1). The superior boundary is the tentorium and the inferior boundary is the cerebellar tonsil and medullary olives. The anterior border is the posterior dural surface of petrous bone and clivus, and the posterior border is the ventral surface of the pons and cerebellum. The medial border is the cisterns of the pons and medulla and the apex is the region of the lateral recess of the fourth ventricle. The lateral opening of the fourth ventricle, the foramen of Luschka, opens into the CPA. Cranial nerves V–XI traverse the cephalic and caudal extent of the CPA. The central structures crossing the CPA to and from the IAC are the facial (CN VII) and vestibulocochlear nerves (CN VIII), respectively.
Figure 61–1.
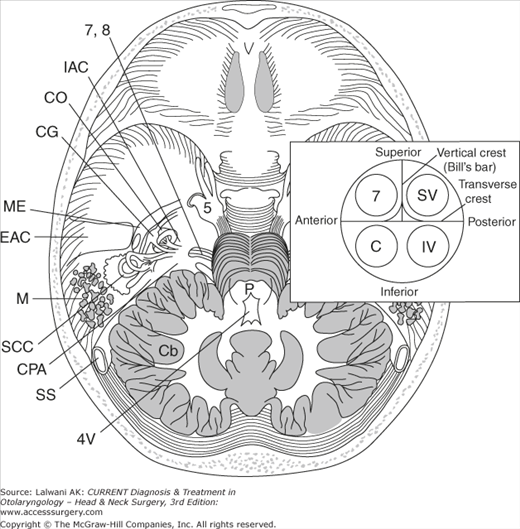
The anatomy of the CPA and its relationship to the temporal bone within the skull is shown. Inset shows the location of the cranial nerves within the IAC: the facial nerve (7) and the cochlear nerve (C) are in the anterior compartment, whereas the superior and inferior vestibular nerves (SV and IV, respectively) are in the posterior half of the IAC. 5, trigeminal nerve; 7, facial nerve; 8, cochlear nerve; IAC, internal auditory canal; CO, cochlea; GG, geniculate ganglion; ME, middle ear; EAC, external auditory canal; M, mastoid; SCC, semicircular canal; CPA, cerebellopontine angle; SS, sigmoid sinus; 4V, fourth ventricle; Cb, cerebellum; P, pons.
Cranial nerves VII and VIII are covered with central myelin provided by neuroglial cells as they cross the CPA and carry a sleeve of posterior fossa dura into the IAC. The transition to peripheral myelin made by the Schwann cells occurs at the medial opening of the IAC. The vestibulocochlear nerve divides into three nerves: (1) the cochlear nerve and (2 and 3) the superior and inferior vestibular nerves in the lateral extent of the CPA or medial IAC. The IAC is divided into four quadrants by a vertical crest, called Bill’s bar, and a transverse crest. CN VII comes to lie in the anterosuperior quadrant and is anterior to the superior vestibular nerve and superior to the cochlear nerve, whereas the inferior vestibular nerve lies in the posteroinferior quadrant and is inferior to the superior vestibular nerve and posterior to the cochlear nerve (see Figure 61–1). The anteroinferior cerebellar artery (AICA) is the main artery in the CPA and is the source of the labyrinthine artery. The labyrinthine artery via the IAC is an end artery for the hearing and balance organs. The AICA has a variable relationship to cranial nerves VII and VIII and to the IAC.
VS originate in the Schwann cells of the superior or inferior vestibular nerves at the transition zone (Obersteiner–Redlich zone) of the peripheral and central myelin. This transition zone occurs in the lateral CPA or medial IAC. Therefore, VS most often arise in the IAC and occasionally in the CPA. These schwannomas rarely arise from the cochlear nerve and are rarely malignant. The propensity to develop from the vestibular nerves may be due to the vestibular ganglion in the IAC having the highest concentration of Schwann cells.
Recent studies have improved our molecular understanding of VS. VS occur as a result of mutations in a tumor suppressor protein, merlin, located on chromosome 22ql2. Merlin is a cytoskeletal protein encoded by the NF2 gene that is necessary for the maintenance of contact inhibition of cellular growth. The formation of VS requires mutations of both copies of the NF2 gene. One functioning merlin protein prevents the formation of VS. Somatic mutations in both copies of the NF2 gene result in sporadic VS. The probabilities of two spontaneous, independent mutations at one locus predict a unilateral VS presenting in the fourth to sixth decades of life.
In contrast, familial VS occurring in NF2 only requires one occurrence of somatic mutation. People with NF2 inherit one mutated merlin protein and one normal merlin protein. A mutation in the normal allele leads to bilateral VS by age 20. Therefore, NF2 is an autosomal recessive mutation at the gene level since disease expression requires mutations in both alleles of the gene, but the inheritance is autosomal dominant (pseudodominant) since inheritance of one mutated allele often leads to a disease state. NF2 is a central form of neurofibromatosis, with affected patients having central nervous system tumors, including schwannomas, meningiomas, and gliomas. Most of these patients develop bilateral VS. In comparison, patients with NF type l (von Recklinghausen disease) have intra- and extracranial tumors, and <5% of these patients develop unilateral VS. Genetic screens for the NF2 mutation have been developed and offer genetic counseling for family members of patients with NF2. The severity of mutation involving the merlin gene in NF2 can predict the severity of disease manifestation.
Hearing loss is present in 95% of patients with VS. Conversely, 5% of patients have normal hearing; therefore, unilateral vestibular or facial complaints without hearing loss do not rule out retrocochlear disease. Of patients with hearing loss, most have slowly progressive hearing loss with noise distortion. Twenty percent have an episode of sudden hearing loss. The improvement of hearing loss with or without treatment does not rule out retrocochlear disease. The level of hearing loss is not a clear predictor of tumor size.
Tinnitus is present in 65% of patients. The tinnitus is most often constant with a high buzzing pitch. This symptom is often not reported by patients because of the focus on the accompanying hearing loss. Similarly, owing to the central compensation for the slowly evolving vestibular injury, patients tolerate and adapt well to the disequilibrium they experience. The majority of patients have self-limiting episodes of vertigo. The disequilibrium is initially mild and constant and often does not prompt a medical visit. Disequilibrium is present in 60% of patients.
Facial and trigeminal nerve dysfunction occurs after the auditory and vestibular impairments. The patients usually have midface (V2) numbness and also often have an absent corneal reflex. The motor supply of the trigeminal nerve of the muscles of mastication is rarely affected. The sensory component of the facial nerve is first affected and causes numbness of the posterior external auditory canal and is referred to as Hitselberger sign. Facial weakness or spasm occurs in 17% of patients and usually leads to a diagnosis of VS within 6 months.
Patients with large VS tumors or tumors that have undergone rapid expansion have visual complaints of decreased visual acuity and diplopia due to compromise of CN II, IV, or VI. Hydrocephalus leads to complaints of headache, altered mental status, nausea, and vomiting and, on examination, increased intracranial pressure and papilledema. Compression of the lower cranial nerves IX and X causes dysphagia, aspiration, and hoarseness, and examination reveals a poor gag reflex and vocal cord paralysis.
Magnetic resonance imaging (MRI) with gadolinium contrast is the gold standard for the diagnosis or exclusion of VS. An MRI scan also allows for surgical planning. The various lesions within the CPA may be differentiated based on their varying imaging and enhancing characteristics. The MRI characteristics of a VS include a hypointense globular mass centered over the IAC on a T1-weighted image with enhancement when gadolinium is added. VS are iso- to hypointense on T2-weighted images (Figure 62–2).
When MRI scans cannot be used or are not accessible, a computed tomography (CT) scan with iodine contrast or an auditory brainstem response (ABR) offers a reasonable alternate screening modality. CT scanning with contrast provides consistent identification of CPA tumors that are larger than 1.5 cm or have at least a 5-mm CPA component. VS appear as ovoid masses centered over the IAC with nonhomogeneous enhancement. CT scans with contrast can miss intracanalicular tumors unless there is bony expansion of the IAC.
The average patient requires 4 y from the onset of symptoms to the diagnosis of VS. The diagnostic dilemma lies in choosing the appropriate patient to undergo audiometric and imaging studies. Most patients present with complaints of unilateral hearing loss or hearing distortion, unilateral tinnitus, vertigo or disequilibrium, and facial numbness, weakness, or spasm. Patients with unilateral auditory, vestibular, and facial complaints need to undergo careful evaluation to rule out retrocochlear disease. The initial step in the evaluation includes an audiology exam. If the audiology exam suggests a retrocochlear lesion, then imaging of the CPA is performed to rule out a retrocochlear lesion. Vestibular testing lacks specificity in diagnosing VS.
The standard auditory evaluation should include pure-tone audiometry, a word recognition score (WRS), acoustic reflex thresholds, and acoustic reflex decay. Pure-tone audiometry of patients with VS shows asymmetric, down-sloping, high-frequency sensorineural hearing loss in almost 70% of patients. The hearing may also be normal, may involve only the low frequency, or may be a flat hearing loss or a trough or peak hearing loss. A retrocochlear-based hearing loss causes WRS scores to be lower than that predicted by the pure-tone thresholds. This out-of-proportion depression of speech intelligibility is further accentuated when retested at a higher speech intensity. This phenomenon is called rollover. A poor WRS is present in about 50% of patients with VS. An abnormal WRS should trigger an imaging evaluation, but a normal WRS does not rule out a VS. A loss of acoustic reflexes or the presence of acoustic reflex decay is present in most cases of VS, but normal acoustic reflexes do not preclude VS.
Vestibular testing does not provide a sensitive or specific means of diagnosing VS. The most common test ordered to evaluate vestibular complaints includes an electronystagmogram (ENG). An ENG in a patient with VS will show a reduced caloric response in the problematic ear. The extent of the vestibular function predicts the amount of postoperative vertigo. The location of the VS on the inferior or superior vestibular nerve may also be predicted by the ENG because the ENG primarily evaluates the lateral semicircular canal innervated by the superior vestibular nerve.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


