10 Vestibular Schwannoma • Sometimes called acoustic neuroma, but is not on the cochlear (acoustic) nerve, nor is it a neuroma • Male = female distribution; typically present 40 to 60 years (younger if neurofibromatosis 2 [NF2]) • Incidence 1/100,000 per year (autopsy studies show up to 0.7% population may have vestibular schwannoma at death) • 95% unilateral, sporadic • 5% bilateral—associated with NF2 • Account for 80% of cerebellopontine angle (CPA) tumours and 6% of all intracranial tumours • May originate from junction of glial and Schwann cells of vestibular nerve, within internal auditory meatus (Obersteiner–Redlich zone) • Haemorrhage can occur in reticular type leading to sudden increase in size • Cystic degeneration possible • NF2—autosomal dominant; aberration on long arm of chromosome 22 leading to defect in tumour suppressor protein merlin (aka schwannomin, neurofibromin 2) • Questioned link with cellphone usage, but evidence not conclusive • Otological phase: small tumour compresses structures in the meatus • Neurological phase: expansion into CPA: – Facial weakness—uncommon (gradual compression allows for compensation as normal number of end plates are innervated by fewer neurons) – Ataxia/unsteadiness—brainstem/cerebellar involvement – Diplopia (VI n)—rare – Hoarseness and dysphagia (IX n, X n)—rare • Magnetic resonance imaging (MRI) scan: non-contrast screening protocols; usually iso/hypointense to brain, hyperintense to CSF on T1 and isointense to slightly hyperintense on T2; best shown with T1 contrast (gadolinium) or FIESTA or CISS (T2-weighted) sequences • (CT with contrast if MRI contraindicated) • Pure tone audiogram: 65% have high-frequency loss • Brainstem evoked response (interaural latency of wave V)—accuracy better for larger tumours (>1.5 cm) • Speech discrimination: “roll-over” seen as intensity increase and optimum discrimination score reduces • Meningioma • VII n neuroma • Cochlear nerve neuroma—rare
10.1 Terminology
10.2 Epidemiology
10.3 Pathology
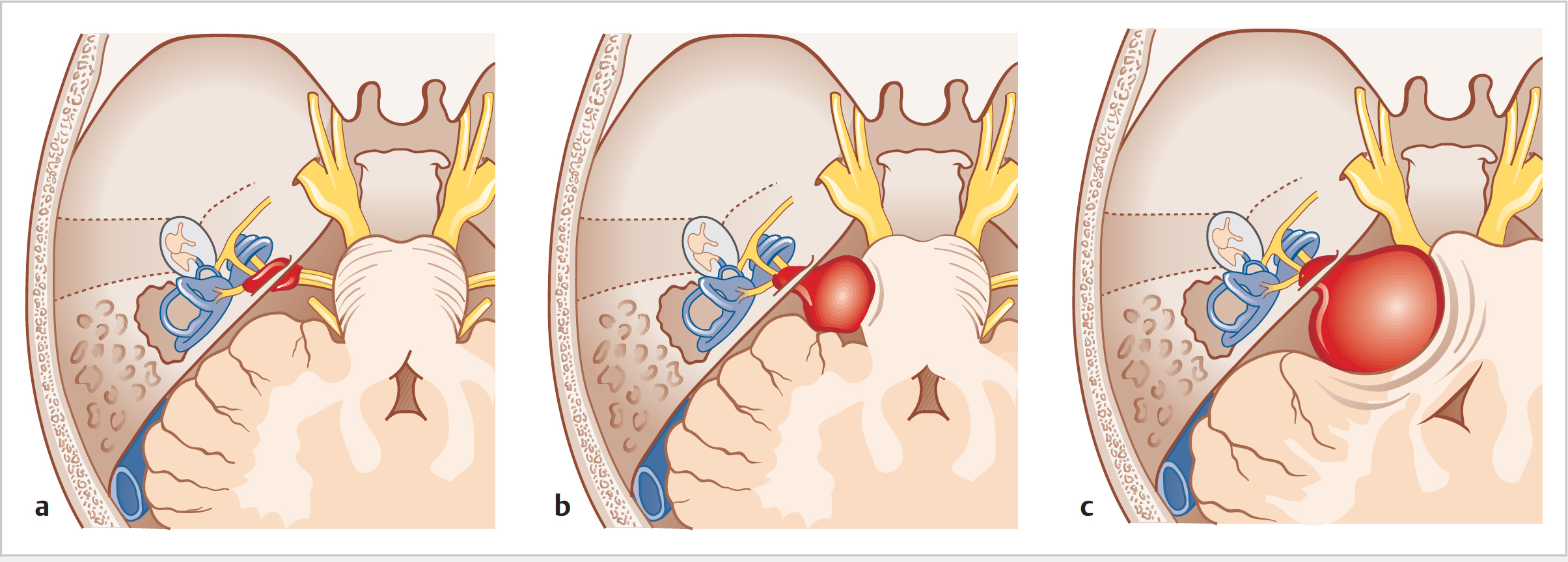
10.4 Clinical Features (Fig. 10.1)
 Gradual and progressive unilateral deafness (90%)—degree of hearing loss (HL) not related to size of tumour
Gradual and progressive unilateral deafness (90%)—degree of hearing loss (HL) not related to size of tumour
 Sudden-onset HL (10%)
Sudden-onset HL (10%)
 Normal hearing (5%)
Normal hearing (5%)
 Associated with unilateral tinnitus (70%)—can be the only symptom
Associated with unilateral tinnitus (70%)—can be the only symptom
 Imbalance unusual unless acutely due to bleed inside tumour (slow compression allows for gradual compensation); dysequilibrium often present with rapid head movements
Imbalance unusual unless acutely due to bleed inside tumour (slow compression allows for gradual compensation); dysequilibrium often present with rapid head movements
 Hitzelberger sign: anaesthesia of medial, posterior, or superior areas of the external auditory canal
Hitzelberger sign: anaesthesia of medial, posterior, or superior areas of the external auditory canal
 Trigeminal nerve symptoms: facial pain, numbness, loss of corneal reflex
Trigeminal nerve symptoms: facial pain, numbness, loss of corneal reflex
 Headache—posterior fossa dura irritation leading to dull aching around ear
Headache—posterior fossa dura irritation leading to dull aching around ear
 Late symptoms
Late symptoms
 Terminal symptoms (raised cerebrospinal fluid or CSF): failing vision (papilloedema), headache, reduced Glasgow coma score; coma
Terminal symptoms (raised cerebrospinal fluid or CSF): failing vision (papilloedema), headache, reduced Glasgow coma score; coma
10.5 Investigations
10.6 Differential Diagnosis of CPA Tumours
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


