4 Otitis Media • Commonly children in between 3 to 7 years of age • Viral (rhinovirus, RSV, adenovirus)—most resolve within 24 hours; or bacterial (Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis) • C/o: fever, rubbing ear, pain, hearing loss (HL); symptoms may improve when tympanic membrane (TM) ruptures/discharge • Predisposing factors include: age (<7 years), non-breastfeeding, day care attendance, race, anatomy (e.g., cleft palate), immunodeficiency • Rx: analgesia; consider antibiotics if failure to resolve after 24 to 48 hours or immediately if age <2 years or systemically unwell • Consider if 3 episodes in 6 months or ≥4 in a year • Treatment options include watchful wait, long-term low-dose antibiotics (e.g., trimethoprim) or grommet insertion • Healed chronic otitis media (COM): healed perforation, tympanosclerosis • Inactive mucosal COM: dry TM perforation, noninflamed middle ear (ME) mucosa • Inactive squamous COM: TM retraction, not retaining debris or infected • Active mucosal COM: TM perforation with mucopus, inflamed ME mucosa • Active squamous COM: cholesteatoma • Termed myringosclerosis when confined to TM • May arise from abnormal healing in response to inflammatory episodes or trauma (e.g., post-myringotomy) • See changes to lamina propria connective tissue component of TM and ME mucosa • Inflammation damages collagen fibres, fibroblasts invade in reparative phase causing excess collagen synthesis and hyalinization; fibres fuse as indistinct mass • Usually asymptomatic; large plaques in TM may cause conductive HL; may cause ossicular fixation in ME • Surgery indicated to prevent discharge/waterproofing; while repair may improve hearing (closure of air–bone gap) it also risks making hearing worse • HL with perforation related to: • Success of surgery may relate to surgeon, eustachian tube (ET) function, smoking, discharging at time of surgery • Traumatic perforations: water exclusion, most heal by 6 weeks • Classification attic retractions (pars flaccida)—Tos • Sadé’s Classification of pars tensa retractions • Rx: most asymptomatic and do not lead to cholesteatoma; watchful wait often best; consider ventilation tube insertion, treatment of sinonasal disease to improve ET function, excision of pocket with grafting (e.g., cartilage) and cortical mastoidectomy to increase air reservoir; little good evidence to support intervention
4.1 Acute, Chronic, and Secretory Acute Otitis Media (AOM)
4.1.1 Recurrent AOM
4.2 Chronic Otitis Media
4.2.1 Various classifications; consider:
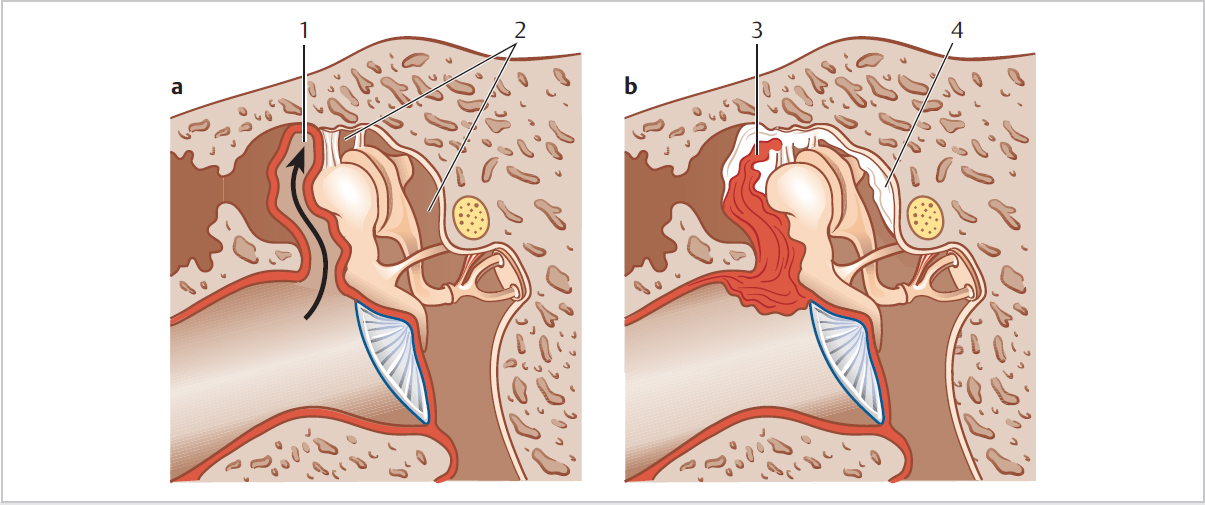
4.2.2 Tympanosclerosis
4.2.3 TM Perforations
 Size
Size
 Loss of baffling effect on round window
Loss of baffling effect on round window
 Reduced ratio of TM: footplate to overcome air:fluid impedance mismatch
Reduced ratio of TM: footplate to overcome air:fluid impedance mismatch
 Associated ossicular chain damage, e.g., if over incudostapedial joint
Associated ossicular chain damage, e.g., if over incudostapedial joint
 Position (umbo involvement = worse hearing)
Position (umbo involvement = worse hearing)
4.2.4 TM Retractions
 I: dimple
I: dimple
 II: onto malleus neck
II: onto malleus neck
 III: bony erosion (of scutum)
III: bony erosion (of scutum)
 IV: keratin accumulation/cholesteatoma
IV: keratin accumulation/cholesteatoma
 I: annular retraction
I: annular retraction
 II: onto long process of incus
II: onto long process of incus
 III: onto stapes/promontory
III: onto stapes/promontory
 IV: adhesive to medial wall
IV: adhesive to medial wall
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


