Vestibular Disorders: Introduction
The value and function of the vestibular system may often be underestimated when considering the various special senses that we possess. However, of all the special senses, unilateral loss of the vestibular system may cause the most significant determent for our daily function and survival. Millions of people present annually to their physician with the complaint of dizziness. The goal of this chapter is to discuss the common disorders that affect the vestibular system and provide a framework for the evaluation, diagnosis, and treatment of patients with vestibular disorders.
Injury to the peripheral or central vestibular system causes asymmetry in the baseline input into the vestibular centers and this causes vertigo, nystagmus, vomiting, and a sense of falling toward the side of the injury. Vertigo is defined as the illusion of movement. However, the chief complaint of patients with injury to the vestibular system is usually not vertigo but dizziness. If the complaint is clarified to be vertigo, the duration, periodicity, and circumstance of the vertigo and the presence of other neurological signs or symptoms allow for categorization of the vertigo.
The proximity of the vestibular system to the auditory system often causes vertigo to be coupled with hearing loss. The role of the otolaryngologist includes clarifying the subset of patients who have vertigo due to injury to the vestibular system and differentiating central from peripheral vestibular disorders. The evaluation includes a complete head and neck and vestibular examination (Table 56–1). The diagnostic evaluation includes audiology, vestibular testing, and imaging. Knowing the duration of the vertigo or disequilibrium and the presence or absence of hearing loss allows for a narrowing of the differential diagnosis (Table 56–2). The vertigo may be due to injury of the peripheral or central vestibular system. Often, the presence of other neurological abnormalities leads to an investigation for a central cause of the vertigo. However, central vestibular injury due to a lesion or stroke may mimic a peripheral vestibular disorder.
|
| Time | No Associated Hearing Loss | Hearing Loss Present |
|---|---|---|
|
|
|
Most patients with peripheral vestibular disorders have benign paroxysmal positional vertigo (BPPV), Meniere disease, or vestibular neuronitis. These patients generally improve with supportive or conservative care (medical or physical therapy). The small percentage of medically recalcitrant patients can then be helped with surgical intervention. The surgical interventions, in general, ablate the vestibular system and rely on central compensation and vestibular rehabilitation to improve the patient’s condition.
The central compensation for vestibular injury occurs via the cerebellum. The cerebellum provides a “clamping” response to the injured vestibular system to reduce the effects of the abnormal vestibular signal. In an acute injury such as vestibular neuronitis, the vertiginous response lasts 3–5 days, and then the central compensation is able to modulate the signal from the injured vestibular system. In episodic injuries, such as Meniere disease, the central compensation is not able to be as effective; therefore, with each new episode, there are acute vertiginous symptoms. In a slowly evolving process such as a vestibular schwannoma, the central compensation occurs in step with the vestibular dysfunction, and the patient may have minimal to no vestibular symptoms. The central compensation is enhanced by vestibular activity and delayed by the prolonged use of medical vestibular suppression. This observation has led to the development of vestibular rehabilitation programs.
Vestibular rehabilitation programs use three strategies: (1) habituation exercises, which facilitate central compensation by extinguishing pathologic responses to head motion; (2) postural control exercises; and (3) general conditioning exercises. Vestibular rehabilitation is critically important in the elderly because their ability to have optimal central compensation is diminished.
Benign Paroxysmal Positional Vertigo
- Sudden vertigo lasting seconds to minutes with head movement
- No associated hearing loss
- Characteristic nystagmus (latent, geotropic, fatigable) with Dix-Hallpike test.
BPPV is one of the most common types of peripheral vertigo, arising as a result of debris in the posterior semicircular canal. Patients complain of vertigo lasting seconds, with no associated hearing loss when in certain positions. The average age of presentation is in the fifth decade and there is no gender bias. The incidence may range from 10 to 100 cases per 100,000 individuals per year. Nearly 20% of patients seen at vertigo clinics are given the diagnosis of BPPV. Ten to fifteen percent of patients have an antecedent history of vestibular neuronitis and another 20% have a history of head trauma.
BPPV occurs because a semicircular canal has debris either attached to the cupula or free floating in the endolymph. The semicircular canal becomes stimulated by the movement of these particles in response to gravity. The study of temporal bones from patients with BPPV showed basophilic deposits adherent to the cupula; this finding was termed cupulolithiasis. Intraoperative findings during posterior canal occlusion in patients with resistant BPPV have shown free-floating debris in the endolymph. Electron microscopy of these particles shows that they are likely otoconia originating from the macula of the gravity-sensitive utricle. This process has been termed canalolithiasis.
The cupula of the semicircular canal has the same specific gravity as the endolymph and so is not sensitive to gravity. However, the debris in the semicircular canal moves in response to gravity and when the patient places the semicircular canal in a dependent position, the particles move and entrain endolymph with them and cause deflection of the cupula. The unexpected gravity-sensitive response from the semicircular canal causes vertigo. The majority of BPPV is due to debris in the posterior canal, but debris may also enter the horizontal and superior semicircular canals.
Patients usually complain of a sudden onset of vertigo that lasts 10–20 seconds with certain head positions. The triggering positions include rolling over in bed into a lateral position, getting out of bed, looking up and back (top-shelf vertigo), and bending over. The vertigo may be associated with nausea. Patients have normal hearing (no new loss), no spontaneous nystagmus, and a normal neurological evaluation.
Imaging is reserved for patients who do not have the characteristic nystagmus, have associated neurological findings, or do not respond to treatment. The imaging choice is a magnetic resonance imaging (MRI) scan with gadolinium contrast to evaluate the brainstem, the cerebellopontine angle (CPA), and the internal carotid artery (IAC). The MRI is the most sensitive and specific test to identify posterior fossa tumors.
Patients should have no new hearing loss. The audiogram should show symmetric hearing with appropriate speech discrimination scores. The tympanogram should be normal. An asymmetric hearing loss calls into question the diagnosis of BPPV and further evaluation is required.
BPPV is diagnosed by observing a characteristic nystagmus when performing the Dix-Hallpike test (Figure 56–1). There is a latency of 1–2 seconds before the onset of the nystagmus and vertigo. The nystagmus is mixed with a torsional and vertical component and is geotropic (down-beating, rotatory nystagmus). The nystagmus follows the Ewald law for excitation of the dependent posterior semicircular canal. The nystagmus is in the plane of the canal, and the fast phase is toward the stimulated canal. The vertigo and nystagmus increase and then decrease within 20 seconds; they are reduced with repeated Dix-Hallpike tests and so the nystagmus is fatigable. All these criteria need to be present to diagnose a patient with BPPV due to debris in the posterior semicircular canal.
Figure 56–1.
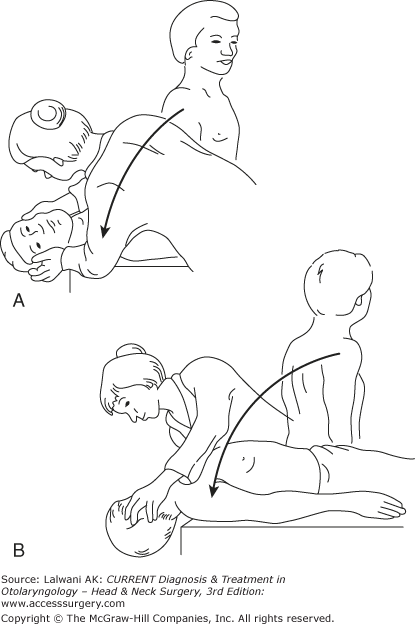
Dix–Hallpike test. (A) For testing the right posterior semicircular canal, the patient sits on the examination table and turns his or her head to the right 45°. This places the posterior semicircular canal in the sagittal plane. The examiner stands facing the patient on the patient’s right side or behind the patient. (B) The patient is then moved by the examiner from the seated to the supine position with the head slightly hanging over the edge of the table. The right ear is down and the chin is pointing slightly up. The eyes are observed for the characteristic nystagmus.
The primary management for BPPV includes maneuvers, Epley (particle or canalith repositioning procedure), and Semont (liberatory maneuver) to reposition the debris into the utricle. The most widely used Epley repositioning maneuvers is depicted in Figure 56–2. The maneuver may be repeated if the patient is still symptomatic. Eighty percent of patients are cured by a single repositioning maneuver. If the symptoms persist after a single maneuver or if patients have recurrent symptoms, the repositioning maneuver may be repeated or patient can be given exercises to perform at home.
Figure 56–2.
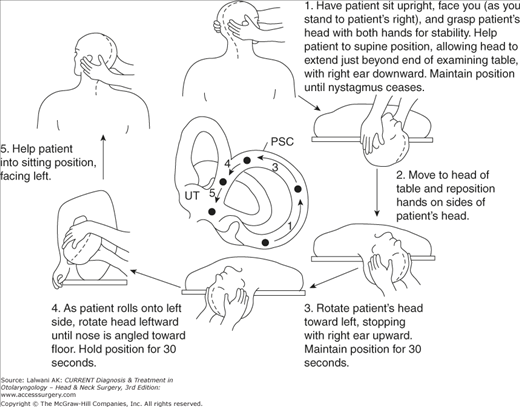
Epley maneuver. The patient is taken through four moves, starting in the sitting position with the head turned at a 45° angle toward the affected side. (1) The patient is placed into the Dix–Hallpike position (supine with the affected ear down) until the vertigo and nystagmus subside. (3) The patient’s head is then turned to the opposite side, causing the affected ear to be up and the unaffected ear to be down. (4) The whole body and head are then turned away from the affected side to a lateral decubitus position, with the head in a face-down position. (5) The last step is to bring the patient back to a sitting position with the head turned toward the unaffected shoulder.
Surgical treatment is available for a very small number of patients with intractable BPPV. These patients have failed repositioning maneuvers and have no intracranial pathology on imaging studies. The primary surgical option is posterior semicircular canal occlusion. A standard mastoidectomy is performed and the posterior semicircular canal is fenestrated. The membranous canal is occluded with muscle, fascia, or bone pate, or collapsed with a laser. The occlusion prevents debris and subsequent endolymph movement to deflect the cupula. There may be a temporary mixed hearing loss that usually recovers. The success rate for an occlusion of the posterior semicircular canal is high. A more technically challenging surgical option with an increased risk to hearing involves ablating the nerve supply of the posterior semicircular canal via a singular neurectomy.
The natural history of BPPV includes an acute onset and remission over a few months. However, up to 30% of patients may have symptoms for longer than 1 year. Most patients improve with a repositioning maneuver. Patients may have unpredictable recurrences and remissions, and the rate of recurrence may be 10–15% per year. These patients may be retreated with a repositioning maneuver. A subset of patients who have adapted by not using certain positions in order to avoid the vertigo or who have other balance disorders can benefit from balance rehabilitation therapy.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


