Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

13

Vertical Deviations
Vertical deviations pose special challenges to the beginning ophthalmology resident as well as to the experienced strabismus surgeon. The muscles involved in vertical deviations are ones that have multiple functions that vary in different fields of gaze. This results in incomitance (variable deviation in different fields of gaze) and adds layers of complexity to the understanding, diagnosis, and management of vertical strabismus. Other complicating factors include the issue of torsion (not a factor when dealing only with horizontal deviations) and the small margin of error from both a cosmetic and a functional viewpoint when treating conditions of vertical misalignment. This is true functionally because normal vertical fusional amplitudes are much smaller than horizontal fusional amplitudes; therefore, a procedure to improve vertical misalignment must be much more precise so that little is left to the fusional vergence mechanisms. Cosmetically, a vertical misalignment is much more noticeable than a horizontal misalignment of similar magnitude because of the changes in the eyelids and palpebral fissures that accompany any vertical strabismus.
Vertical strabismus remains a difficult topic to organize, and we have chosen to separate it into congenital and acquired disorders, further categorizing it by the major division of paralytic versus mechanical. As this is a text of pediatric ophthalmology, we have not discussed disorders that are seen purely or primarily in adults.
 Congenital Vertical Strabismus
Congenital Vertical Strabismus
Paralytic Vertical Strabismus
Superior Oblique Muscle Palsy
Paresis of the fourth cranial nerve (to the superior oblique muscle) is the most common cause of a paretic vertical deviation in childhood. Many strabismologists find that superior oblique paresis is the most common cause of a vertical strabismus at all ages. Although unilateral paresis is more common than bilateral, a bilateral palsy may be masked by asymmetry and only become manifest when treatment is instituted for one side.
A patient with a congenital superior oblique palsy presents either with a head tilt and/or face turn (to the opposite side) to compensate for the vertical misalignment or, if the patient does not have binocular fusion, without a compensatory head posture but with a manifest hypertropia of the affected side. Soon after onset (i.e., early in childhood for a congenital etiology), the hyperdeviation is frequently greatest in the field of action of the involved superior oblique muscle (i.e., down and to the left for a paretic right superior oblique). As time passes, the ipsilateral inferior oblique muscle, the direct antagonist of the paretic superior oblique, begins to overact, and the hyperdeviation may be greatest in its field of action (i.e., up and to the left for a paretic right superior oblique) (Fig. 13-1C). Later, spread of comitance may be seen as the hyperdeviation spreads to other fields of gaze, and precise diagnosis of the original palsy becomes difficult.
The wide range of possible patterns that can be observed in a patient with a superior oblique paresis led Knapp to propose a classification scheme for superior oblique muscle paresis depending on which fields of gaze manifested the greatest vertical deviation. Knapp’s classification is still in use today and is helpful in assessment of motility and in planning for surgery. This classification should not be memorized but rather understood as an approach to management by directing surgery to the muscles, that act in the fields of greatest deviation (Fig. 13-2).1,2
There are four consequences of a palsy of an extraocular muscle.3 For the case of the superior oblique, these include (1) underaction of the paretic muscle (superior oblique), (2) over-action of the antagonist to the paretic muscle (ipsilateral inferior oblique), (3) secondary overaction of the yoke muscle of the other eye when the paretic eye is fixating (contralateral inferior rectus), and (4) inhibitional palsy of the contralateral antagonist (contralateral superior rectus).
Despite the spread of comitance, it is usually possible to diagnose a superior oblique paresis by the three-step test that utilizes this information as well as the Bielschowsky head tilt phenomenon.4–6
Three-Step Test
The three-step test is an attempt to find a single cyclovertical muscle palsy. It is not useful if the problem is a restrictive one or if more than one muscle is weak.
Step 1: Determine which eye is hypertropic in the primary position (done by cover testing) (Fig. 13-3). As an example, we will say that the right (R) eye is hypertropic. This being the case, the paretic muscle is therefore either a depressor of the hypertropic eye (R superior oblique or R inferior rectus) or an elevator of the hypotropic (contralateral) eye (L inferior oblique or L superior rectus). At this point, the involved muscle has been narrowed from eight possibilities to four.
Step 2: Determine whether the deviation is greater in gaze R or L (Fig. 13-4). In our example, we will say that the deviation is greater in left gaze. The paretic muscle is the muscle whose field of action corresponds to the side in which the deviation is greater (R superior oblique or L superior rectus). At this point, the involved muscle has been narrowed from four possibilities to two.
Step 3: Determine whether deviation is greater in head tilt to the R or L (Fig. 13-5). Let us say that the deviation in our example is greater in right head tilt. When the head is tilted to one side (e.g., to the right), the ipsilateral eye must in tort (right) and the contralateral eye must extort (left). The two superior muscles (superior oblique and superior rectus) are the intorters. If the ipsilateral superior oblique is paretic, the superior rectus of that side performs all or most of the intorsion. The superior rectus, however, also elevates the eye, and this elevation is unopposed by the paretic superior oblique whose function is to depress the eye. Therefore, if the deviation increases with head tilt to the same side, then the ipsilateral superior oblique is paretic (R superior oblique); if the deviation is greater with head tilt to the opposite side, the contralateral superior rectus is paretic. At this point, the involved muscle has been identified by a process of elimination (Fig. 13-6).7
The presence and degree of torsion can be helpful in the diagnosis and management of superior oblique paresis. Subjective extorsion can be measured most readily by the double Maddox rod test. The Bagolini striated glasses and the synoptophore and/or the Lancaster red-green projection test (done with bars of light rather than circles) are other options.
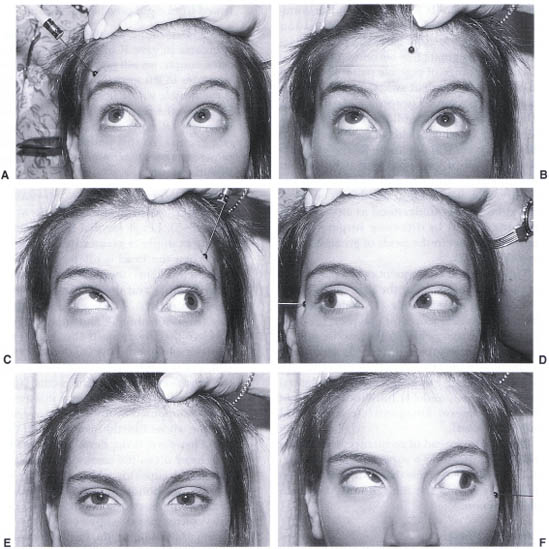
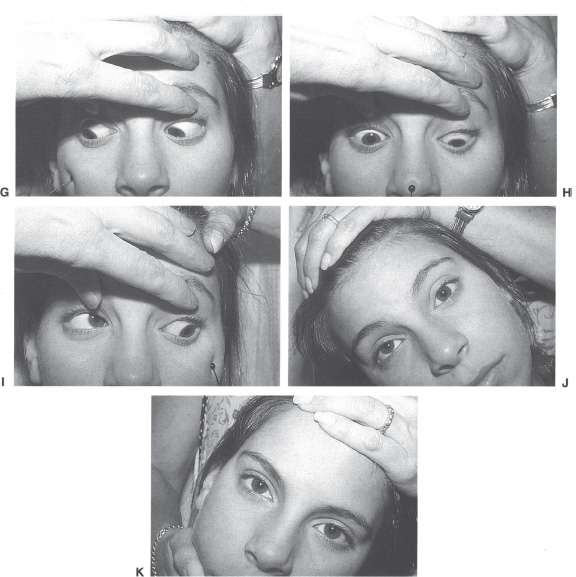
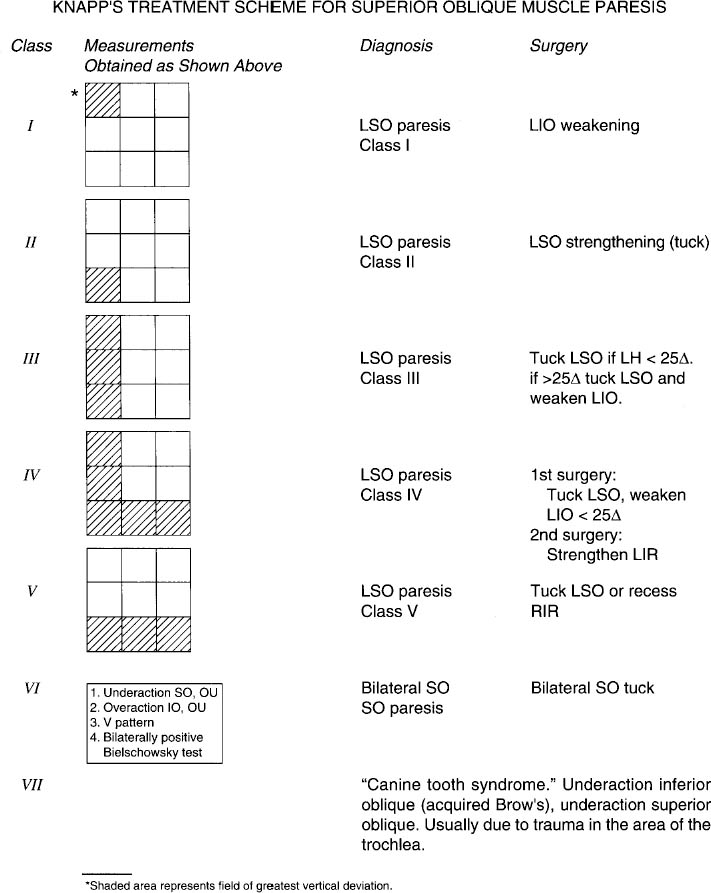
FIGURE 13-2. Knapp’s classification and treatment scheme for superior oblique muscle paresis.
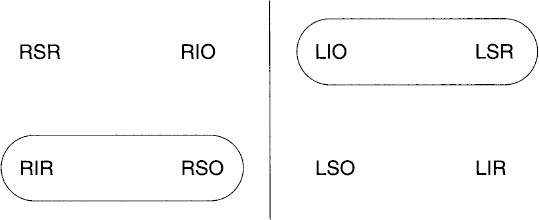
FIGURE 13-3. Three-step test. Step 1: Decide which eye is higher in primary gaze (in this example, the right eye). Circle the muscles that could cause a hypertropia on that side (i.e., depressors of right eye [RIR or RSO] or elevators of left eye [LIO or LSR]).
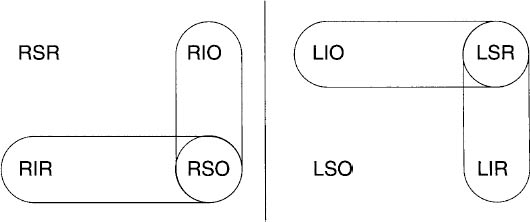
FIGURE 13-4. Three-step test. Step 2: Decide whether the deviation is greater in gaze R or L (in this example, deviation is greater in left gaze). Circle the muscles whose field of action corresponds to the side in which the deviation is greater (i.e., RSO, RIO or LSR, LIR). At this point, the involved muscle has been narrowed from four possibilities to two (because only two muscles are circled twice).
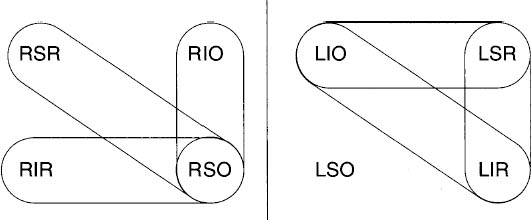
FIGURE 13-5. Three-step test. Step 3: Decide whether the deviation is greater in head tilt to the R or L (in this example, deviation is greater in right head tilt). Circle the muscles whose field of action corresponds to the side in which the deviation is greater (i.e., RSR, RSO or LIO, LIR). (See text for more detail on why these are the muscles involved.) At this point, the involved muscle has been identified by a process of elimination (the RSO, this is the only muscle circled three times).
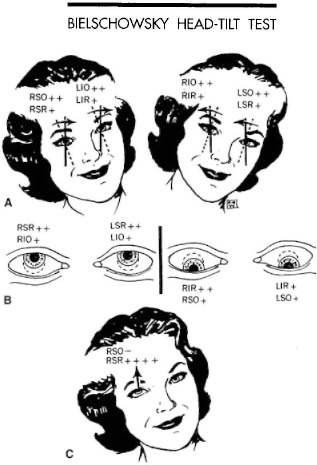
FIGURE 13-6. Bielschowsky head tilt test.7 Physiologic principles: (A) When the head is moved around an anteroposterior axis, compensatory eye movements occur around an anteroposterior axis of the globe because of reflex innervation originating in the otolith apparatus. Thus, when the head is tilted to the right, the right superior oblique and rectus muscles contract to provide incycloduction of the right eye. In the left eye the left inferior oblique and rectus muscles contract to effect excycloduction of that eye. Analogously, cycloductions occur in the opposite direction when the head is tilted to the left. The compensation of the head inclination by wheel rotations of the eyes is incomplete and does not fully offset the angle of inclination. (B) Muscles that act synergistically during cycloductions become antagonists when elevating and depressing the globes. Under normal conditions, however, the vertical action of the rectus muscles exceeds that of the oblique muscles; conversely, the effect of the oblique muscles on cycloductions is greater than that of the vertical rectus muscles. (C) When the head is tilted toward the involved side in a case of right superior oblique paralysis, the vertical and adducting action of the RSR is unopposed. Contraction of this muscle in an attempt to incycloduct the eye results in an upward movement of the right eye (positive Bielschowsky head tilt test), thus increasing the vertical deviation. (From von Noorden,52 with permission.)
Objective extorsion can be assessed by examination of the fundus by indirect ophthalmoscopy. The presence of extorsion is further evidence for a superior oblique paresis (although its absence does not rule out the diagnosis) and must be taken into consideration when deciding on a surgical plan.4
As discussed previously, a superior oblique paresis is most often congenital. In many cases the patient will deny a previous problem and presents as an adult with diplopia secondary to a decompensated congenital paresis. Evaluation for a compensatory head posture (which the patient may not recognize) and review of old photographs (which may show a head tilt) are good evidence for a congenital etiology (Fig. 13-7). Facial asymmetry from longstanding ocular torticollis may be present and, some studies suggest, may be at least partly reversible if early surgical intervention is undertaken to correct the compensatory head posture. Large vertical fusional amplitudes also speak to a congenital etiology.
When not congenital, the second most common etiology for a superior oblique paresis is traumatic. A history of head trauma should be elicited if possible, but may not have been severe enough to cause this problem. The fourth cranial nerves decussate at the roof of the midbrain and are particularly susceptible to traumatic injury (hemorrhage) in this area, which may lead to bilateral superior oblique weakness.8 In adult patients, when not congenital or traumatic, a microvascular etiology may be the cause. If none of these etiologies can be identified as the cause, neurological evaluation with neuroimaging is indicated to rule out the possibility of neoplasm or other acquired disease of the brainstem or orbit.
The Fixing Eye
If the patient maintains fusion through a compensatory head posture, there may not be a “fixing eye.” However, if there is a manifest deviation, there will be a fixing eye. If the fixing eye is the nonparetic eye, the surgery should be undertaken on the paretic eye (often addressing a contracture of the inferior oblique from longstanding unopposed overaction). If the fixing eye is the paretic eye, surgery can be undertaken on either eye as determined by other factors.
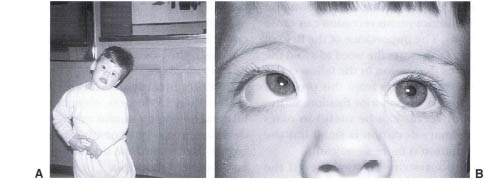
FIGURE 13-7. (A) Young boy demonstrates a large left head tilt due to a congenital right superior oblique palsy. (B) Same child demonstrates a large right hypertropia in left gaze.
Treatment
Prisms. Prisms may be used occasionally in the treatment of superior oblique paresis, particularly during the observation period for an acquired deviation while the diagnosis is being solidified and the stability of the deviation is observed. Incomitance, the presence of torsion, and the magnitude of the deviation are often factors that prevent the utility of prisms on a long-term basis; however, in unusual cases, prisms can be the sole means of therapy.
Surgery. Surgery is indicated in children (or adults) to relieve an anomalous head posture or diplopia. There is debate in the literature regarding whether early surgery for congenital superior oblique paresis can prevent or ameliorate the development of facial asymmetry. In longstanding deviations, it is wise to aim for a small undercorrection because the patient has built up large fusional vergence amplitudes to control the hypertropic eye and will easily compensate for a small residual deviation but has no mechanism to deal with a hypertropia of the opposite eye as would occur with an overcorrection.
Depending on the clinical picture (and evaluating which fields of gaze have the greatest deviation—as outlined by Knapp2), the surgery indicated may be a strengthening of the ipsilateral superior oblique, a weakening of the ipsilateral inferior oblique, or a weakening of the contralateral inferior rectus. Less commonly, a weakening of the ipsilateral superior rectus or strengthening of the ipsilateral inferior rectus may be needed. A combination of these procedures may be performed in one patient either simultaneously or sometimes sequentially in a staged fashion.
In young children who present with a superior oblique paresis, a floppy, redundant, or missing tendon may be found.9 Helveston classifies the anatomic abnormalities found in superior oblique paresis and underlines the importance of assessing the tendon at the time of surgery to perform the most appropriate surgical procedure.10 Plager recommends exaggerated traction testing as a means to identify a floppy or missing tendon.11 Many authors recommend a superior oblique tuck for children who demonstrate a floppy tendon.12 Parks advocates a superior oblique tuck for children with anomalous head tilt.
More typically, a floppy tendon is not found, and the most important surgical principle is to operate on the muscles acting in the fields of greatest deviation.2 Commonly, a large overaction of the ipsilateral inferior oblique may be present with a large deviation up and to the opposite side. In such cases, a weakening procedure of the inferior oblique is indicated.
If there is a large deviation down and to the opposite side, this can be addressed with either a strengthening procedure of the ipsilateral superior oblique or a weakening of the contralateral inferior rectus (the yoke muscle of the paretic superior oblique). Deciding between these two options should take into account the presence and magnitude of a torsional component (more torsion favors the superior oblique procedure) and the magnitude of the deviation in down gaze (if there is little or no down gaze deviation, an inferior rectus recession can cause overcorrection). The importance of the field of down gaze also underlines the need to avoid the addition of poor depression in the fellow eye to an eye that already suffers from this problem. The use of a Faden, or posterior fixation, suture of the inferior rectus can be useful in cases where the primary deviation is small but the down gaze deviation is more significant.
These procedures can be combined if the deviation is largest in all fields of gaze opposite to the affected eye. More often the ipsilateral inferior oblique and contralateral inferior rectus procedures are combined because operating on the inferior and superior obliques of the same eye may result in an iatrogenic “Brown’s” syndrome (decreased elevation in adduction). Weakening of the ipsilateral inferior oblique muscle will correct up to approximately 15 prism diopters (pd) of hypertropia. Inferior rectus weakening contributes an additional ~ 3pd per mm of recession and in older, cooperative patients is often performed on an adjustable suture. If more correction is needed, attention is turned to additional muscles on an individualized basis applying the same principles as outlined previously.
If the deviation also is present in gaze up and to the same side, the ipsilateral superior rectus can be weakened. If present in gaze down and to the same side, the ipsilateral inferior rectus can be resected. These procedures can be added as necessary to the previously detailed options.
If there is no significant hyperdeviation in primary position, but there is torsional diplopia and the presence of significant extorsion as measured with double Maddox rod testing, a Harada-Ito procedure is indicated.13 This procedure is an anteriorization and temporal advancement of the anterior fibers of the superior oblique tendon. This is indicated because the anterior fibers are responsible for intorsion and the posterior fibers for depression.
Bilateral Superior Oblique Paresis
Although these may be traumatic, bilateral superior oblique pareses can also be congenital. Sometimes surgery to correct a seeming unilateral problem “unmasks” a paresis of the opposite side due to significant asymmetry. A classic bilateral case manifests a left hyperdeviation on right gaze and a right hyperdeviation on left gaze. Signs that should raise suspicion of bilaterality include measurable extorsion of greater than 15 degrees, objective evidence of bilateral torsion on fundus exam, reversal of the deviation in any gaze or tilt position (particularly in gaze toward the side of the paretic eye), and V-pattern esotropia.14
Bilateral surgery may be indicated for bilateral superior oblique paresis and often consists of bilateral inferior oblique weakening or superior oblique strengthening procedures. Asymmetry can be addressed by titrating the amount of surgery done to each side and/or by the addition of a single inferior rectus recession when indicated.
Double Elevator Palsy
As Wilson points out,9 “double elevator palsy” is a misnomer; he suggests replacing the term with monocular elevation deficiency (MED). Double elevator palsy implies a paresis of both the inferior oblique and the superior rectus muscles of one eye, but, in fact, these patients may have deficient elevation due to inferior rectus restriction or to paresis of just one of the elevator muscles. We agree with this appropriate change in terminology. It is unlikely that one muscle innervated from the superior division and one muscle innervated from the inferior division of the third cranial nerve would be selectively paretic in so many cases.
Incidence
Although the incidence of this disorder is unknown, it is documented less frequently among series of general pediatric ophthalmology patients and appears to be present more often in studies of congenital ptosis populations.9,15–17 It may be even more frequent in patients with the Marcus-Gunn jaw-winking phenomenon.18
Findings
The patient presents with a monocular deficiency of elevation of the involved eye. The elevation deficit is often worse in abduction, helping to distinguish this disorder from Brown’s syndrome in which there is deficient elevation in adduction. There may be a hypotropia in primary gaze that increases in upgaze. When fixating with the uninvolved eye, the affected eye will be hypotropic and often ptotic (this may be true ptosis, pseudoptosis, or a combination of both) (Fig. 13-8). When fixating with the affected eye, a large hypertropia will be seen in the uninvolved eye. A chin-up head position may be adopted to maintain fusion. Horizontal strabismus and amblyopia are not uncommon and should be evaluated. Bell’s phenomenon is absent in restrictive and infranuclear paretic cases but may be preserved in supranuclear cases.
Etiologic Subtypes
The first type of MED is due to elevator muscle paresis. Forced ductions are normal with no evidence of restriction. Force generation and saccadic velocity testing are consistent with a paretic etiology. True ptosis is often present. Bell’s phenomenon may be preserved if the paresis has a supranuclear etiology or missing if the cause is infranuclear (such as superior division third nerve palsy or absent muscle).9 Many authors feel that the true etiology of this subtype of MED may be a solitary superior rectus palsy, which over time has exhibited spread of comitance through all superior fields of gaze. This would be consistent with the view that the superior rectus is the principle elevator not only in abduction and primary gaze but also in adduction.19 Additionally, at least one case has been documented to have normal electromyography of the inferior oblique muscle.
The second type of MED is due to inferior rectus restriction. Forced ductions are positive. Saccadic velocity testing is normal. Active force in the superior rectus may be felt when the eye is held in depression with forceps. This type of MED is more common than the paretic type and may not have a primary gaze hypotropia.20
The third type of MED is a combination of both types. Long-standing elevator paresis leads to contracture of the inferior rectus muscle. Forced ductions are mildly positive. Saccadic velocity to upgaze is slowed, and ptosis may be present or absent.9
Treatment
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


