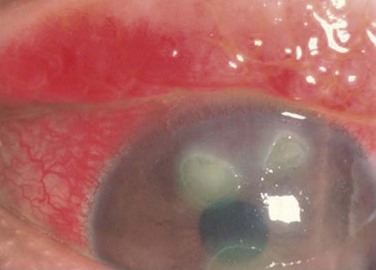
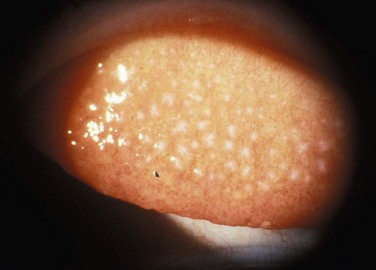
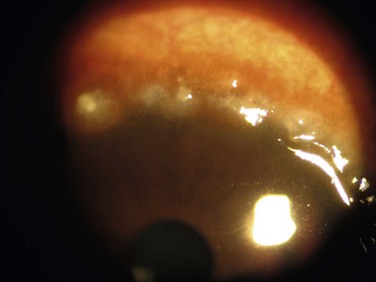
14 Vernal Keratoconjunctivitis (VKC) is an allergic ocular surface disease that affects primarily the conjunctiva and cornea and is characterized by chronic ocular surface inflammation. The chronicity of VKC can lead to debilitating ocular surface disease, with myriad potential complications, that may permanently affect vision. The name ‘vernal’ itself implies spring and youth, reflecting two common characteristics of VKC. It primarily affects children, although it may rarely occur in adults. In addition, the disease course is often seasonal with exacerbations in the warmer months (typically the spring), but in some patients it can become a chronic condition and occur throughout the year.1 Males are affected more than females; however, one series reports a female preponderance in cases.2 The diagnosis of VKC is clinical and is based on typical signs and symptoms. The classic signs include conjunctival hyperemia, tarsal papillae, limbal papillae, and ropy mucous discharge. Symptoms of VKC are itching, photophobia, and tearing. There may also be pain if the cornea is involved. The disorder is found with varying frequency in all geographic areas, but has a higher incidence in warmer climates. VKC has been described in the ophthalmic literature for over 150 years. The condition has been referred to in the literature by many names, including spring catarrh, phlyctaena palladia, circumcorneal hypertrophy and conjunctivitis verrucosa, but the current nomenclature of vernal keratoconjunctivitis is now almost universally used.3 The precise etiology and pathogenesis of VKC are still unknown. There have been many clinical and laboratory studies performed in recent years in an attempt to answer these questions. While it is established that VKC is an IgE- and Th2-mediated allergic condition, it is clear that the simplified concept of a type I allergic hypersensitivity reaction does not fully describe the complex immune process involved in VKC.4–6 VKC may affect the superior palpebral conjunctiva, the bulbar conjunctiva, or both, with patients exhibiting two forms of disease: palpebral vernal and limbal vernal. The inferior palpebral conjunctiva is less often involved with VKC. In the palpebral form, the superior tarsal conjunctiva is the primary location of pathology, making ptosis a common associated finding of palpebral VKC. Papillae of various sizes develop on the superior tarsal conjunctiva (Fig. 14.1). As the disease progresses, the papillae may coalesce into larger lesions referred to as ‘cobblestone’ or ‘paving-stone’ papillae (Fig. 14.2). Deep furrows are seen in between the papillae. These large papillae may cause mechanical damage to the cornea. The discharge is thick and ropy and characteristically has a dirty white or cream color. Microscopic examination of the discharge shows large numbers of eosinophils, mononuclear, and polymorphonuclear inflammatory cells.1 Scarring of the conjunctiva is not seen in VKC. Figure 14.1 Slit lamp photograph of the upper tarsal palpebral conjunctiva, demonstrating a diffuse papillary reaction. Figure 14.2 Giant papillae of the upper tarsal palpebral conjunctiva. The classic cobblestone appearance of VKC. In the limbal form, there is a broadening and opacification of the limbus. This can produce a semitransparent, thickened appearance of the limbus. These signs are often seen first in the superior limbus, but can spread 360 degrees. Discrete yellow or gray nodules may appear in the thickened limbus. In severe cases, these nodules can become confluent. White, punctate lesions known as Horner–Trantas dots may develop in the hypertrophied limbus (Fig. 14.3). Figure 14.3 Slit lamp photograph of Horner–Trantas, dots characteristic of limbal vernal keratoconjunctivitis. Either form of VKC can affect the cornea, with the earliest corneal manifestation typically found as a superficial punctate keratitis, referred to as keratitis of Tobgy.1 It can progress to multiple, discrete, dull gray points of epithelial irregularity and degeneration, which stain with fluorescein or rose bengal. These spots may become confluent and coalesce into a corneal erosion or ulcer, referred to as a vernal shield ulcer (Fig. 14.4). The ulcer is typically indolent, characteristically oval in shape, and most commonly found in the upper half of the cornea. The ulcer is often shallow with white edges. A grayish opacification of Bowman’s membrane may develop which will eventually harden into a gray plaque in the base of the ulcer. Often, plaque removal is needed to promote healing of the ulcer. After an ulcer is healed, corneal neovascularization and scarring are often seen.1,7 Another potential complication of the shield ulcer is secondary bacterial or fungal infection by colonized pathogens.8 Another corneal manifestation of VKC is pseudogerontoxon, which resembles a segment of arcus senilis or gerontoxon, and is seen in many individuals with limbal VKC. The lesion is typically found a few millimeters anterior to the limbus in the midperipheral cornea and is often arcuate in pattern. It may be unifocal or multifocal (Fig. 14.5). It is an important clinical finding because pseudogerontoxon is often the only clinical evidence of previous allergic eye disease.9 Vernal keratoconjunctivitis is predominantly a disease of children and adolescents. Two large case series from central Italy, where there is a relatively high incidence of VKC, have reported the mean age at diagnosis as between 6.8 ± 5years and 11 ± 5years.10,11 Only 4% of newly diagnosed patients were older than 20 at the time of initial diagnosis.10 There are more males with VKC than females. Multiple case series have reported a male to female ratio of approximately 3 : 1.10,11 Interestingly, the higher number of males affected seems to only be present in children and adolescents. When looking at adults with VKC over the age of 20 years, the male to female ratio is 1 : 1.11 Estrogen and progesterone receptors are present in the epithelium and subepithelium of patients with VKC, while not normally present in healthy epithelium. The role these hormonal receptors play in VKC is not known.12 The prevalence of vernal keratoconjunctivitis varies by geographic region. The disease is most prevalent in warm climates. In geographic regions with temperate seasonal change, a relapsing pattern of VKC is often seen, with flare-ups occurring in the spring and summer months, and remission of symptoms in the cooler winter months. In climates that remain hot all year round, a perennial form of VKC is commonly seen. This is not an absolute finding, and individual patients with either relapsing or perennial VKC are seen in any climate. The estimated overall prevalence of VKC is 3.2/10 000 across all of western Europe. A higher prevalence is seen in Italy (27.8/10 000) where the climate is warmer, while a lower prevalence of VKC is seen in Norway (1.9/10 000) where the climate is cooler.13 Since VKC is an allergic condition, other allergic co-morbid conditions may be associated. A family history of atopic disease is seen in 48% of patients with VKC.11 Among patients with VKC, 15–64% also have asthma, 30–49% also have allergic rhinitis, and 16–24% also have eczema.10,11 Not all patients with VKC have co-morbid conditions. VKC is the only clinical issue in 59% of patients.11 Allergen skin prick testing for common allergens is positive in 44–58% of VKC patients. Specific serum IgE levels are positive in 57% of VKC patients,10 and are increased in VKC patients compared to serum IgE levels in normal controls.11 Other than allergic conditions, keratoconus is the disease most commonly associated with VKC. Prevalence of clinical keratoconus in VKC patients is 2–9%. In a large cohort of patients with VKC, 27% were identified as having keratoconus based on videokeratography maps.14 Eye rubbing, which is common among patients with VKC, due to chronic eye itching, has been proposed as an explanation for the high rate of keratoconus in this cohort.15 Iatrogenic cataracts from steroid use, as well as steroid-induced glaucoma complications, have been reported. Bacterial keratitis and shield ulcers are seen in 10% of patients with VKC and these are typically the most severe cases. Fungal keratitis is rare, but has been reported in VKC.16 To date, no specific genotype has been demonstrated to have a relationship with vernal keratoconjunctivitis. Current research is investigating this question. The presence of eosinophilia, increased expression of cytokines, and other cellular mediators, including increased CD4 lymphocyte cells in the epithelium and subepithelium of affected patients suggests VKC may be associated with up-regulation of the cytokine gene cluster on chromosome 5q. This gene regulates production of IL-3, -4, -5, granulocyte/macrophage-colony-stimulating factor (GM-CSF), type 2 T-helper cells, growth of mast cells and eosinophils and production of IgE, all of which are seen in the pathology of VKC.17 The classic and most constant clinical symptoms of vernal keratoconjunctivitis are itching, redness, photophobia, and tearing; these are all seen in > 90% of patients with VKC.11 The tarsal form of the disease is the most common, with superior tarsal papillae seen in 44–83% of patients. Limbal papillae are seen in 8–11%, and a mixed clinical picture is found in 9–46% of patients with VKC. Giant cobblestone papillae occur in 16% of patients.10,11,14 Ninety-eight percent of cases are bilateral.11 Other common signs include Horner–Trantas dots in 15% of reported cases and mucous discharge in 53% of reported cases.11 Treatment of VKC is guided by the severity of symptoms. The response to treatment is variable. In one case series, with long-term follow up of greater than 3 years, 27% of patients had a complete resolution, 35.4% showed improvement but mild to moderate persistence of symptoms, and 32% had no change in signs or symptoms as a response to therapy. Severe worsening involving visual loss is rare and is seen in cases with ulcerative keratitis. 6% of patients had a loss of two or more lines of best corrected vision due to corneal scarring and neovascularization.11
Vernal Keratoconjunctivitis
Vernal Keratoconjunctivitis

Demographics
Prevalence
Co-Morbid Conditions
Genetics
Clinical Features
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine