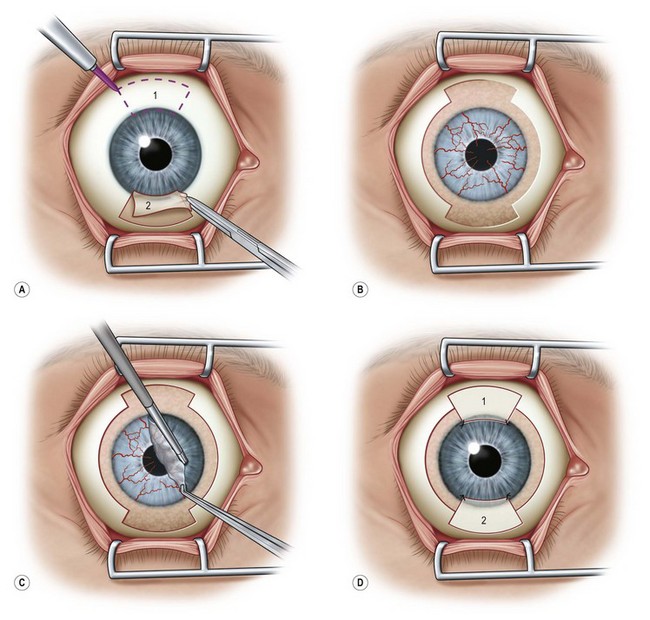
41 Harvesting the donor tissue is essentially the same as in CLAU. This procedure is typically done under local anesthesia using subconjunctival injection of xylocaine plus epinephrine. In some cases, retrobulbar/peribulbar anesthesia may be necessary. Two 60-degrees arcs of limbal lenticule, each spanning 2–3 clock hours, are harvested from one or both eyes of donor at 12 or 6 o’clock positions. A gentian violet surgical marking pen may be used to mark the conjunctival portions of the grafts (Fig. 41.1). The dissection can be started with lamellar dissection from the corneal side approximately 1 mm anterior and extending 2 mm posterior to the limbus, leaving behind the Tenon’s capsule as much as possible. Alternatively, as the authors prefer, the dissection can be started on the conjunctiva and carried forward towards the limbus about 1–1.5 mm onto the cornea in a superficial manner. Care should be taken to avoid buttonholing of the donor tissue. Dissection onto the peripheral cornea past the palisades of Vogt is critical in order to obtain limbal stem cells. Amputation of the tissue peripheral to this landmark with result in the harvesting of conjunctiva only. Typically, a 5-mm conjunctival skirt is harvested; however, the amount of the conjunctiva can be increased if the recipient eye also requires symblepharon repair and fornix reconstruction. After excising the donor tissue, the surrounding conjunctiva is undermined and advanced anteriorly and sutured with 10-0 nylon (or dissolvable suture) to close or partially close the conjunctival defect. Although the donor sites heal quickly, closing the defect enhances patient comfort and reduces likelihood of localized pannus formation.1 The surgical procedure of lr-CLAL is identical to CLAU.1 Surgery is done under general or retrobulbar/peribulbar anesthesia. After a 360-degree conjunctival peritomy, subconjuntival scar tissues are removed as much as possible, which typically results in the recession of the conjunctival edge to 3–5 mm from the limbus. Hemostasis is achieved with mild wet-field cautery or dilute epinephrine (1 : 10 000). Corneal pannus is removed with special caution not to perforate the cornea. Donor grafts are sutured to the recipient eye at the corresponding anatomic sites by interrupted 10-0 nylon sutures. As an alternative to using sutures, the lr-CLAL grafts can also be directly fibrin glued onto the prepared bed.2,3 This approach has the potential to decrease operative time, increase ease of technique, and improve patient comfort postoperatively. The surgical site may be covered with an overlain amniotic membrane or a high-DK bandage contact lens. At the end of surgery, upper and lower punctal occlusion and lateral tarsorrhaphy may be performed to protect grafts from the mechanical trauma of blinking, as well as from evaporative moisture loss in the early postoperative period in the more severe cases (Fig. 41.2).
Living-Related Conjunctival–Limbal Allograft (lr-CLAL) Transplantation
Surgical Procedure
Recipient Eye
Living-Related Conjunctival–Limbal Allograft (lr-CLAL) Transplantation