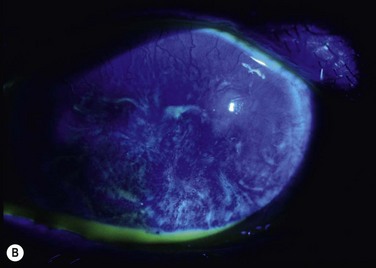
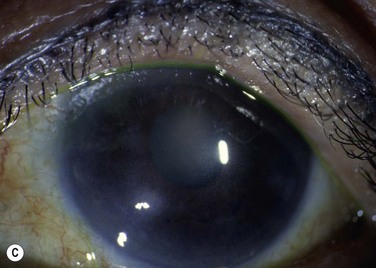
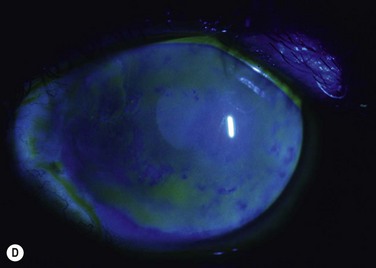
40 In a discussion at the Cornea World Congress in 1964, José Barraquer described the use of an autograft of limbus from the unaffected eye in cases of superficial burns as a preparatory procedure before keratoplasty.1 He noted that this improved the state of the corneal epithelium but the mechanism was not discussed. In 1966, Strampelli et al. reported two cases of improvement in vascularized opaque corneas with transplantation of a complete ring of limbus from the other eye.2 They described the technique in more detail at the Second International Corneo-Plastic Conference in London in 1967.3 It was not until some time later that the role of the limbus as the niche for the stem cells responsible for the corneal epithelium was elucidated, and Kenyon and Tseng reported on the use of autografts of conjunctiva and limbus for management of diffuse unilateral limbal deficiency in 1989.4 Conjunctival limbal autografts (CLAU) were described within a classification system for epithelial transplantation proposed by Holland and Schwartz in 1996.5 Since then, there have been many reports describing the use of limbal autografts, and the role of CLAU in management of unilateral ocular surface disease has been comprehensively reviewed.6–9 Clinical signs of limbal deficiency include varying combinations of conjunctivalization of the cornea, with associated vascularization and fibrovascular pannus, persistent or recurrent epithelial defects and scarring or stromal haze.9 Symptoms include poor vision, chronic or recurrent discomfort and photophobia. Probably the most common use of limbal autografts has been in surgery for pterygium in the form of an ipsilateral limbal translocation, though there is little evidence that the limbal part of the autograft adds any benefit over a standard conjunctival autograft.10 In most other forms of unilateral limbal deficiency the autograft is harvested from the other eye. In this situation, a unilateral chemical injury is probably the most common clinical scenario. Figure 40.1 demonstrates improvement in the ocular surface with CLAU after chemical injury. It has been recognized that the state of the rest of the ocular surface is critical to the outcome of limbal transplantation. Preoperative assessment must include thorough examination of the ocular adnexa and ocular surface. The nature of chemical injuries and many of the other causes of limbal deficiency is such that other ocular surface or adnexal problems are commonly associated. Two important considerations in determining management are whether the condition is unilateral or bilateral and whether there is conjunctival involvement.5 Lid malposition, symblepharon, and trichiasis all need to be dealt with prior to limbal transplantation. The most common pre-existing problem is that of dry eye and this is a major prognostic factor.11 If aqueous tear function is inadequate, then punctal occlusion should be performed. Blepharitis or ocular surface inflammation should be controlled optimally before surgery if possible.
Conjunctival Limbal Autograft
Introduction
Indications
Preoperative Assessment and Considerations
Conjunctival Limbal Autograft