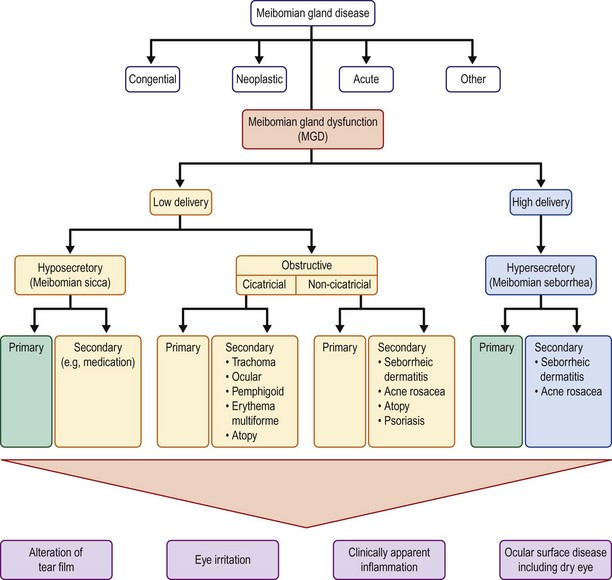
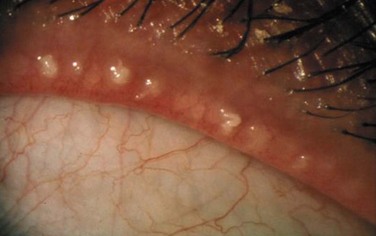
6 The first line of defense is the eyelashes, which collect debris, therefore preventing it from interacting and damaging the surface of the eye. There are roughly 100 lashes in the upper lid and 50 in the lower lid.1 The layers of the eyelid, from superficial to deep, include the skin, orbicularis muscle, tarsus, and palpebral conjunctiva. The eyelid’s primary function is to protect the ocular surface, but they also function in cleansing and lubricating the eye. With each blink, the tear film is continuously spread over the ocular surface, maintaining optical visual clarity of the cornea. The subconscious blink reflex occurs every 6–10 seconds, and it has also been determined that significant restoration of the ocular surface occurs during extended times of closure, such as sleeping. The conjunctiva is an ectodermally derived mucous membrane that extends from the mucocutaneous junction of the eyelid margins to the corneoscleral limbus.2 The conjunctival surface reflects onto the palpebral surfaces, creating fornices and folds, which allow for movement of the globe. Nasally, the plica semilunaris is formed by the folding of the conjunctiva. The conjunctival epithelium must be kept continuously moist to avoid desiccation.3 The conjunctival epithelium is rich in goblet cells, which are mucin-producing cells critical for the tear film. At the corneoscleral junction, the conjunctiva forms radial folds called the palisades of Vogt. The conjunctiva is also the sole source of lymphatic tissue of the eye, and therefore, has an important function in regard to protection against infection. The final structure of the ocular surface is the cornea, which serves as the transparent window of the eye, allowing light rays to pass into the eye to be processed by the visual system. To accomplish this, the cornea must have a normal contour and be avascular, transparent, and be essentially dehydrated. The corneal epithelium is continuous with the conjunctival epithelium and both are composed of nonkeratinized, stratified, squamous epithelium cells. The corneal epithelium is 50 µm thick and has five or six layers of three different types of cells: superficial cells, wing cells, and basal cells. It is believed that the corneal epithelium is replaced by a population of stem cells found at the anatomical limbus.4 The corneal epithelium completely sheds and renews itself approximately every 7 days. The corneal epithelium is not a mucus membrane; however, it is susceptible to desiccation if not properly protected by the lids and tear film. The lacrimal functional unit (LFU) has been described as an encompassing term representing the integrated system that comprises the ocular surface (cornea, conjunctiva, accessory lacrimal and meibomian glands), the main lacrimal glands, the blink mechanism that spreads tears, and the sensory and motor nerves that connect them whose parts act together and not in isolation.5 Poor function of this unit will often result in dry eye disease. The critical relationship and dependence of the lid–lash complex to the ocular surface is described above. If the eyelid margin is not apposed to the corneal surface, significant ocular surface inflammation and mechanical trauma can occur. Flaws in the lid–lash complex, which can lead to instability of the ocular surface are myriad, but fall into two basic groups. One group leads to a mechanical rubbing and irritation of the ocular surface and the other is related to poor closure resulting in desiccation of the tissue. Disorders such as trichiasis, distichiasis, epiblepharon, lid imbrication syndrome, and entropion, cause ocular surface problems through the mechanical rubbing of lashes against the conjunctival and corneal surfaces. It is not only the trauma of the lashes rubbing, but also the induced chronic, low-grade inflammation, which further exacerbates the disease process. Most eyelid malpositions involve the lower lid. Trichiasis is distinguished from an entropion or epiblepharon by evaluating the lash orientation when the lid is in its normal position. Trichiasis refers to the condition where the lashes emerge from their normal anterior lamellar origin but are misdirected. Distichiasis is different from trichiasis in that the lashes originate from the more posterior meibomian gland orifices. Both conditions can be congenital or acquired. Another cause of mechanical trauma to the ocular surface creating significant inflammation is floppy eyelid syndrome. In this condition, the rubbery and floppy upper lid is everted during sleep and rubs on the pillow or sheets. This mechanical irritation creates a prominent papillary reaction on the upper palpebral conjunctiva, as well as punctate keratopathy on the cornea. Floppy eyelid is bilateral in 78% of patients, but can be asymmetric. Common external findings include a markedly elongated and lax upper lid and eyelash ptosis of the upper lid (Fig. 6.1). Patients often complain of ocular irritation, mucous discharge, and papillary conjunctivitis6 (Fig. 6.2). There are also reports of an association between keratoconus and floppy eyelid syndrome. One study reported 18% of their patients with floppy eyelid have clinical keratoconus and possibly up to 71% may have subclinical keratoconus.7 Other disorders such as lagophthalmos, eyelid retraction, and ectropion cause damage to the ocular surface by exposure. In these cases, incomplete closure of the lids allows for local increased tear film evaporation and subsequent corneal and conjunctival desiccation. Closure of the eyelids is primarily a function of the upper lid, with the lower lid exhibiting very little upward movement during closure. As a result, many patients tolerate lower lid retraction and scleral show with minimal symptoms, if the upper lid function is normal.8 Resultant inflammation will cause further insult to the ocular surface. Medical management to stabilize the ocular surface and reduce inflammation is important, but often the critical step is surgically addressing the abnormal lid position. Blepharitis is a broad term used to describe inflammation of the lid as a whole. Anterior blepharitis is defined as inflammation of the lid margin anterior to the gray line and centered on the lashes. Marginal blepharitis refers to inflammation of the lid margin and includes both anterior and posterior blepharitis. Posterior blepharitis describes inflammation of the posterior lid margin, which may have different causes, including MGD, conjunctival inflammation, and acne rosacea.9 McCulley et al., in 1982, published six categories for blepharitis, with the first three describing anterior blepharitis and the final three posterior blepharitis and meibomian gland abnormalities. Anterior blepharitis is commonly associated with staphylococcal disease, as well as seborrhea, and presents with inflammation, crusting, and collarettes on the lashes.10 Hyposecretory MGD results from decreased meibum secretion without obvious obstruction. Hyposecretory MGD is seen clinically with gland atrophy and dropout. Contact lens wear has been associated with a decrease in the number of functional meibomian glands.9 Obstructive MGD is a result of obstruction of the duct, resulting in reduced delivery of meibum to the ocular surface. The gland orifice epithelium can become keratinized, creating a low-delivery state. Obstructive MGD is probably the most common form of MGD. Obstructive MGD is further divided into cicatricial and non-cicatricial. The cicatricial form of obstructive MGD results when the duct orifices are dragged posteriorly into the mucosa, as compared to non-cicatricial MGD where the ducts are obstructed but in their normal anatomic position. Causes of cicatricial obstructive MGD include trachoma, ocular cicatricial pemphigoid, erythema multiforme, and atopic eye disease. Non-cicatricial obstructive MGD may be caused by Sjögren’s syndrome, seborrheic dermatitis, acne rosacea, atopy, and psoriasis9 (Fig. 6.3). High-delivery, hypersecretory MGD is defined by the release of a large volume of lipid at the lid margin that is easily visible on examination with digital pressure on the glands. Seborrheic dermatitis has been reported to be associated with hypersecretory MGD in 100% of cases.9 Other causes include acne rosacea and atopic disease. In acne, increased sebum excretion on the face is a critical factor in the disease process9 (Fig. 6.4). The prevalence of MGD reported in the ophthalmic literature varies widely from as low as 3.5%11 to almost 70%.12 One of the challenges of identifying a true prevalence is its wide range of symptoms and clinical findings, creating a broad spectrum that has significant overlap with other ocular surface disorders, specifically dry eye disease. One consistent finding has been the increased prevalence in the Asian population. Several studies12,13 have reported higher than 60% for the Asian population, compared to between 3.5%11 and 19.9%14 for Caucasians.
Classification of Ocular Surface Disease
Introduction
Eyelids and Eyelashes
Lid Margin and Meibomian Glands
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine