TABLE 37-1 Vascular Tumors of the Orbit: Hamartomas | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Ultrasound | CT | ||||||||||
Lesion | Test(s) if Suspect | IR | IS | SA | Typical | Calcification | MRI (Compared to Gray Matter) | Angiography | Encapsulated | Natural History | Management |
Infantile capillary hemangioma | Clinical diagnosis ± enhanced MRI | High and low | Irregular | Moderate | Well-defined to irregular margins; intraconal/extraconal; moderate to intense enhancement ± globe indentation ± orbital bony enlargement | No | T1: Isointense | Multiple feeding vessels ICA, ECA | No | Complete resolution up to 60% age 4 y and 76% age 7 y | ± Oral propranolol ± Intralesional steroids ± Systemic steroids, surgery, cryotherapy, laser, interferon, selective arterial embolization |
Cavernous hemangioma | Enhanced CT | High | Regular | Moderate | Oval or rounded intraconal mass; progressive homogeneous or inhomogeneous enhancement ± globe indentation ± orbital bony enlargement | Rarely | T1: Isointense T2:Hyperintense Spread pattern | Not indicated | Yes | Slowly enlarge | ± Surgical excision |
Orbital vascular malformations | |||||||||||
• No flow/lymphatic | Unenhanced MRI | Low | Regular | Marked | Poorly defined intraconal/extraconal mass with rim enhancement ± global indentation ± orbital bony enlargement | Yes | T1: Hypointense ( lymphatic cyst) Hyperintense ( hemorrhagic cyst) T2: Hyperintense | No | Slowly enlarge until adulthood; spurts of growth with RTI and hemorrhages | ± Sclerotherapy ± Surgical debulking | |
• Venous/venous lymphatic | Spiral CT MRI | Low | Regular | Minimal | Dilated/lobular uniform enhancement | Yes, 45% | Uniform enhancement T1: Hyperintense T2: Hyperintense | Essential prior to surgery | No | Slowly enlarge | ± Sclerotherapy ± Embolization ± Surgery |
• Arterial flow | MRA ± Angiography | Irregular rapidly enhancing mass | Rapid enhancement | Essential prior to surgery | No | Slowly enlarge | ± Embolization with surgery | ||||
IR, internal reflectivity; IS, internal structure; SA, sound attenuation; ICA, internal carotid artery; ECA, external carotid artery; RTI, respiratory tract infection. | |||||||||||
TABLE 37-2 Vascular Tumors of the Orbit: Neoplasias | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Ultrasound | CT | ||||||||||
Lesion | Test(s) If Suspect | IR | IS | SA | Typical | Calcification | MRI (Compared to Gray Matter) | Angiography | Encapsulated | Natural History | Management |
Hemangiopericytoma | CT or MRI ± cerebral angiography | Low to medium | Regular/slightly irregular | Mild to moderate | Oval or rounded extraconal superior mass; intense early enhancement ± orbital bone erosion | Yes | T1: Isointense T2: Isointense Heterogeneous enhancement | Intense blush; multiple feeding vessels | Pseudocapsule | Aggressive local behavior ± distant metastases | ± Surgical excision |
Malignant hemangioendothelioma | CT or MRI ± cerebral angiography | Irregular | Circumscribed or infiltrative orbital mass; intense early enhancement ± orbital bone erosion | Pseudocapsule | Aggressive local behavior ± distant metastases | Surgical excision | |||||
Vascular leiomyoma | Enhanced MRI | Intraconal mass | T1: Isointense T2: Hyperintense | Yes | Slowly enlarge | Surgical excision | |||||
Kaposi’s sarcoma | Clinical ± fluorescein angiography | No | Slowly enlarge | ± Surgical excision, cryotherapy, radiotherapy Intralesional chemotherapy Systemic chemotherapy | |||||||
Epithelioid hemangioma | Excision ± radiotherapy | ||||||||||
Kimura’s disease | No | Surgical excision ± radiotherapy | |||||||||
IR, internal reflectivity; IS, internal structure; SA, sound attenuation; ICA, internal carotid artery; ECA, external carotid artery; RTI, respiratory tract infection. — | |||||||||||
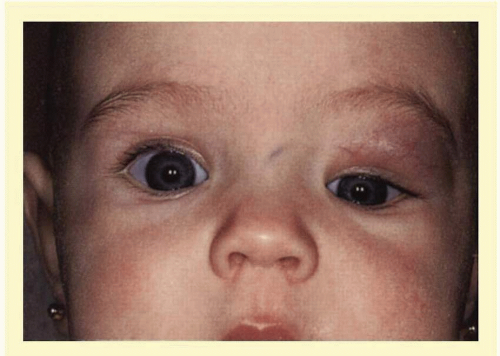 FIG. 37.1 Capillary hemangioma. Eight-month-old patient with a diffuse subcutaneous lesion of the left superior orbit, with a component deep to the orbital septum. Note the displacement of the globe inferiorly. (Courtesy of Dr. Nancy A. Tucker, University of Toronto.) |
 FIG. 37.2 Capillary hemangioma. Six-month-old patient with a circumscribed, red, dimpled dermal “strawberry nevus” capillary hemangioma. This patient had resolution of the induced astigmatic anisometropic refractive error after one intralesional steroid injection. |
 FIG. 37.3 A: Patient with capillary hemangioma at age 2 months. B: Patient at age 5 months, 8 weeks after intralesional steroid injection. Note the stellate areas of pale scarring (herald spots) characteristic of the resolution phase of this lesion. |
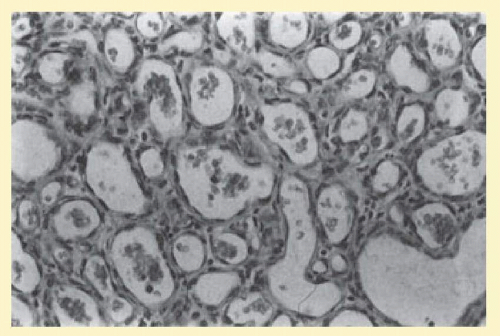 FIG. 37.4 Infantile capillary hemangioma. Characteristic pattern of masses of plump endothelial cells organized into a network of basement membrane-lined vascular channels with small, irregular lumina. Red blood cells are present within these spaces (H&E, ×250). |
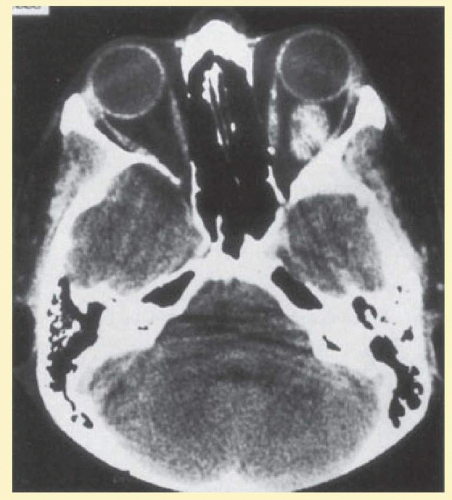 FIG. 37.5 Cavernous hemangioma. Contrast-enhanced axial CT scan shows a well-demarcated, oval intraconal mass in the lateral part of the middle third of the orbit. Note the enhancement within the lesion, which in this instance is inhomogeneous, but can also be homogeneous. |
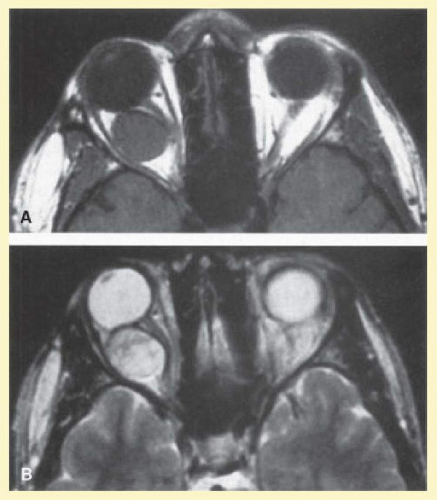 FIG. 37.6 Cavernous hemangioma. Axial MRI demonstrates a well-defined, homogeneous intraconal mass that is isointense to muscle and gray matter on T1-weighted image (A), and hyperintense on T2-weighted image (B). Note the displacement of the optic nerve and indented posterior globe. |
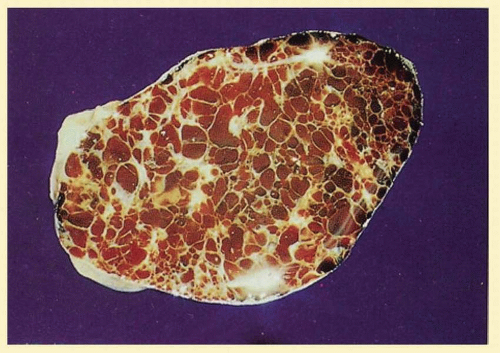 FIG. 37.7 Cavernous hemangioma. Gross cut specimen showing large blood-filled spaces separated by fibrous septa and surrounded by a fine capsule. (Courtesy of Dr. Seymour Brownstein, University of Ottawa.) |
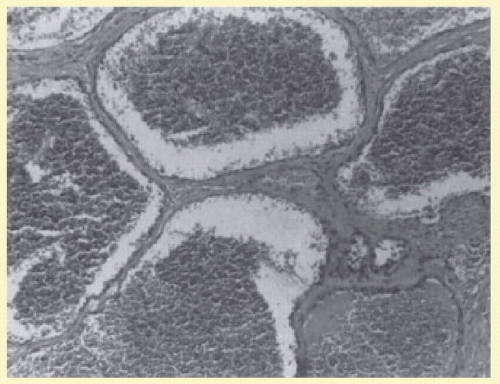 FIG. 37.8 Cavernous hemangioma. Histopathologic appearance of the widely dilated vascular spaces filled with red blood cells. Abundant, loosely distributed smooth muscle is present in the vascular walls, and scattered inflammatory cells can be seen (H&E, ×100). |
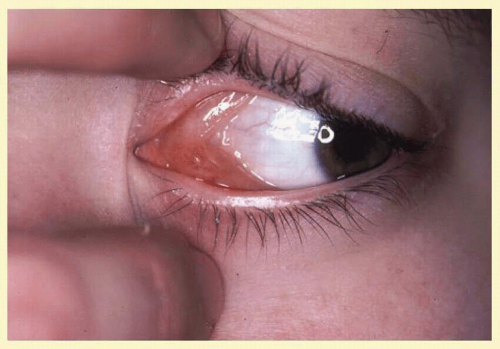 FIG. 37.9 No flow/lymphatic malformation of the orbit. Conjunctival mass with multicystic structures containing serous fluid and an admixture of blood and blood products. (Courtesy of Nancy A. Tucker, MD, University of Toronto.) |
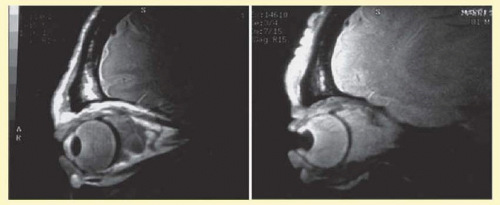 FIG. 37.10 A and B: No flow/lymphatic malformation of the orbit. Sagittal MRI showing dilated cystic spaces hypointense to muscle on T1-weighted images (A) and hyperintense to muscle on T2-weighted images (B). |
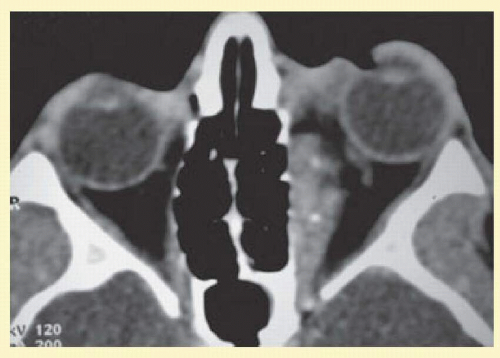 FIG. 37.11 Axial CT scan of patient in Figure 37.9, showing poorly defined orbital mass with calcifications. (Courtesy of Nancy A. Tucker, MD, University of Toronto.) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


