Until recently, the literature for surgical management of uveitis dealt with the many failures due to the complications of surgical inflammation preoperatively, intraoperatively, and postoperatively. One reason for the lack of success had been the viewpoint that uveitis is a single disease cluster compounded by the concept that the diagnosis of uveitis can be determined only with the greatest difficulty. There were no special surgical procedures or even major modifications of standard techniques for handling cataract, glaucoma, retinal detachment, or vitreous opacifications in the patient with uveitis.
Remarkable progress has been made recently. Using a systematic diagnostic approach, the general ophthalmologist should be able to diagnose properly up to 80% of patients with uveitis. Precise uveitic diagnosis is a necessary first step before surgical intervention is considered. Depending on the diagnostic category, the uveitis often responds in a different but predictable manner to surgical intervention. We know this very certainly for cataract extraction. Thus, patients in one category (e.g., those with Fuchs heterochromic iridocyclitis) should be treated differently from those in another category (e.g., those with sarcoidosis) to increase the chances of success. A discussion of the choice of procedures and the modifications of those procedures for the individual cataract entities follows. Interestingly, even the use of intraocular lenses (IOLs), which has undergone intensive investigation, has shown that certain uveitic entities can be candidates for IOL placement while others certainly are not. Great strides have been made in dealing with the very fragile and friable retinal detachment caused by cytomegalovirus (CMV) retinitis as a frequent complication of the acquired immunodeficiency syndrome (AIDS). Many studies have shown that in the small but significant number of patients in whom retinal detachment occurs with this disease, pars plana vitrectomy and injection of 1,000-centistoke or 5,000-centistoke silicon oil can reattach the majority of these retinas. Pars plana vitrectomy can be used to clear the optic media and manage fibrovascular proliferation and proliferative vitreoretinopathy on an inflammatory basis, remove foreign bodies, analyze microorganisms and pathologic cells in the vitreous, and treat retinal detachment. It is of increasing benefit in the treatment of uveitis.
GENERAL MEASURES
Before initiating surgery on patients with uveitis, some general factors must be considered because they may influence the decision of whether to operate, what procedure to use, and what medical measures to take preoperatively, during surgery, and postoperatively.
Surgery should be undertaken when the eye has been free of uveitic activity for a prolonged period. The best time is after the active inflammatory phase of the uveitis has burned out. If this is not practical, the next best time is when the uveitis has been inactive for several months without treatment with corticosteroids. If even this is not possible, then corticosteroids or even immunosuppressives should be used to quiet the eye as much as possible for at least a month before surgery.
If the primary inflammatory site is the anterior uvea, surgery through a posterior approach may be preferable. Conversely, if the primary inflammatory site is posterior, an anterior approach is optimum.
Uveitic entities that have little or no tendency to develop anterior or posterior synechiae (e.g., pars planitis, Fuchs heterochromic iridocyclitis) respond to surgical intervention much better than “sticky” uveitic entities (e.g., sarcoid, chronic iridocyclitis of juvenile rheumatoid arthritis).
Acute, recurrent uveitic eyes handle surgery better than chronically uveitic eyes. Uveitis in association with a markedly low intraocular pressure (IOP) (prephthisical), especially in the absence of a cyclitic membrane, may indicate that the eye is a poor surgical risk.
The use of preoperative, operative, and postoperative local, systemic, and/or periocular corticosteroids allows the uveitic eye to tolerate intraocular surgery better.
TREATMENT OF BAND KERATOPATHY
All eyes with long-standing uveitis may have band keratopathy.1 This is especially true in eyes with juvenile rheumatoid arthritis, uveitis from Toxocara canis, phthisis (Fig. 64.1), or due to long-standing intraocular silicone oil used for retinal detachment surgery. To manage band keratopathy, chelating agents are used to remove the calcium deposits in the basal layers of the epithelium and in Bowman membrane. Before the chelating agent is applied, the overlying epithelium should be removed with diluted alcohol, knife-blade scraping, or other techniques. A dilute solution of sodium ethylenediaminetetraacetatic acid (EDTA; Endrate) is then applied to the cornea.
The procedure is performed with the aid of an operating microscope. After a topical anesthetic is applied, a lid speculum is placed and the epithelium is removed with a dilute solution of alcohol and a blade. A vial of sodium EDTA is diluted 1:50 with sterile balanced salt solution and applied with a sponge to the area of the band keratopathy. The chelating agent is dabbed on the cornea, not irrigated into the eye. This prevents the toxic effects of the chelating solution from injuring other ocular structures. It may take several minutes to determine whether the deposit has been chelated sufficiently to be removed with gentle scraping. If it has not been loosened sufficiently, a more concentrated solution of the chelating agent—up to a dilution of 1:10—may be used. After the procedure has been completed, an antibiotic solution, a cycloplegic, and a semipressure patch are applied to allow the epithelium to heal. Occasionally, a bandage contact lens may be necessary if there is delayed healing of the epithelium.
PENETRATING KERATOPLASTY IN UVEITIS
A wide variety of corneal problems are associated with ocular inflammation, the most significant of which is corneal scarring caused by herpes simplex keratouveitis. Keratoplasty can be performed in these cases if the eye is uninflamed.2, 3 Studies have shown a significant recurrence of herpes in corneas after penetrating keratoplasty, but the longer the eye has been uninflamed before surgery, the better the prognosis. Therefore, in cases of active corneal and intraocular inflammation, penetrating keratoplasty should not be performed until the eye has remained quiet without medication for several months.
The usual indications for visual rehabilitation should be present. Once the eye has been quiet a reasonable length of time, the standard surgical procedure can be followed. Peripheral iridectomies should also be performed in these previously inflamed eyes. Lamellar keratoplasty in patients with herpetic scars and iridocyclitis is rarely indicated. In other forms of corneal opacification associated with ocular inflammation, the eye also should be as uninflamed as possible before keratoplasty.
Conjunctival flaps may play a role in the management of chronic, indolent, noninfectious herpetic disease. Although the bandage contact lens has revolutionized therapy for indolent ulcers recalcitrant to healing, a conjunctival flap may be indicated in such patients or in those in whom a contact lens has been ineffective.
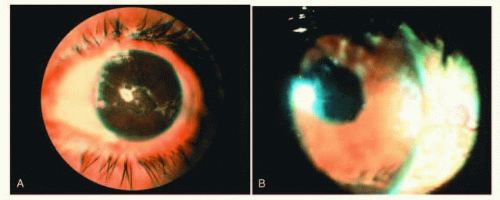
FIG. 64.1 A: A 27-year-old white woman with phthisical eye, band keratopathy, secluded fibrosed pupil, and dense cataract due to juvenile rheumatoid arthritis (shown by ultrasonography). B: After removal of band keratopathy and lensectomy-vitrectomy, the vision improved from light perception to 20/80 (6/24), with a rise in IOP from 2 to 8 mm Hg. The eye is microphthalmic.
UVEITIC GLAUCOMA
Secondary glaucoma, one of the serious complications of intraocular inflammation,4, 5 occurs with various syndromes and may be difficult to manage. Most patients respond poorly to surgery. It is of primary importance to determine the severity of the inflammation and, if possible, the syndrome associated with it. Management includes treatment of the underlying inflammation and of the glaucoma/elevated IOP itself. Various mechanisms produce secondary glaucoma, and it is important to identify them to institute the appropriate therapy.
Clinical Features
In addition to the signs and symptoms of the underlying inflammation is an elevation of the IOP. If there is corneal disease or diffuse edema, the McKay-Marg tonometer (tonometer pen) or pneumotonometry may be needed to measure the IOP. Gonioscopy can determine whether there are synechiae or precipitates in the angle.
Pathology
The trabecular meshwork may be blocked with inflammatory cell debris or frank peripheral anterior synechiae. Iris bombé, posterior synechiae, or rubeosis is also apparent in some cases.
Differential Diagnosis
Table 64-1 gives a list of some of the major uveitic syndromes with which secondary glaucoma can be associated. Glaucoma may occur in any case of severe iridocyclitis, whatever the specific syndrome. Glaucoma secondary to peripheral anterior synechiae may develop late when the inflammation is no longer active.
TABLE 64-1 Uveitic Syndromes with Which Glaucoma May Be Associated
The Posner-Schlossman syndrome or glaucomatocyclitic crisis is characteristically intermittent with little evidence of inflammation.6, 7 Precipitates in the angle, however, may elevate the IOP considerably. Rubella, herpes zoster, and herpes simplex are often accompanied by an elevation of pressure with relatively little anterior chamber inflammation. These diseases are accompanied by characteristic changes in the cornea and skin. Glaucoma occurs in up to 50% of patients with Fuchs heterochromic iridocyclitis.4
Etiology
The two most common causes of secondary glaucoma/elevated IOP in patients with uveitis are severe inflammation with blockage of the trabecular meshwork and peripheral anterior synechiae with secondary angle closure (Table 64-2).
Treatment
Special consideration should be given to the management of acute intraocular inflammation with elevated IOP. If it is certain that corticosteroids are not the cause of the elevated pressure, the following medications can be used alone or in combination to control both IOP and inflammation.
A strong topical corticosteroid four times a day to every hour during the day and every 2 hours during the night. Steroid ointments can be utilized in patients unable to administer drops when sleeping.
A β-blocker such as timolol maleate 0.5% solution one to two times a day.
An α2-agonist such as brimonidine tartrate 0.1%, 0.2% two or three times a day.
Topical carbonic anhydrase inhibitors such as Dorzolamide 2%, Brinzolamide 1% two to three times daily.
Prostaglandin analogs such as Latanoprost 0.005%, Bimatoprost 0.01%, or Travoprost 0.004% can be utilized. Caution should be exercised with use of prostaglandins due to the potential to exacerbate inflammation.
Acetazolamide, 250 mg every 8 hours or 500 mg Sequel every 12 hours.
Cycloplegics administered three or four times per day.
Systemic oral prednisone, 40 to 60 mg daily, if inflammation is severe. GI prophylaxis should be given with
all oral steroids. Caution in diabetic patients with uncontrolled blood sugars.
A sub-Tenon capsule injection of moderately longacting corticosteroid (such as Triamcinolone Acetonide 1%) is used.
TABLE 64-2 Secondary Glaucoma: Causes, Incidence, and Treatment
Miotics are usually contraindicated in acute inflammatory glaucoma. There is some evidence that prostaglandins may aggravate ocular herpes, worsen inflammation, and cause cystoid macular edema. Their use in patients with uveitis is controversial. On the other hand, most ocular inflammations with acute secondary glaucoma due to blockage of the angle by inflammatory cells improve after just a few days of corticosteroid therapy. Prostaglandin and prostamine therapy has been noted to increase iris pigment, epithelium pigmentation, conjunctival injection, and to a lesser degree, increase inflammation in the eye. There is evidence that Xalatan 0.005% (Pharmacia & Upjohn Company, Kalamazoo, MI), in particular, may worsen herpetic anterior inflammation, and hence this use should be avoided in patients with uveitis.
Corticosteroid-induced glaucoma is a major differential diagnostic problem when it complicates intraocular inflammation. Typically, the IOP does not elevate until at least 4 to 6 weeks after the corticosteroid therapy is begun. It should be noted that IOP elevation has occurred in patients prior to 4 weeks after beginning steroid therapy and careful monitoring schedules followed in patients at risk for optic nerve damage. If the inflammation responds well to the corticosteroid drops, sub-Tenon capsule and subconjunctival depot preparations should be avoided. Frequently, the clinician must balance the benefit conferred by the corticosteroid against the eye’s limited ability to tolerate elevations of pressure. If the glaucoma cannot be controlled, it may be necessary to remove a previously injected depot preparation surgically. Elevated IOP is frequently seen after anterior sub-Tenon or subconjunctival placement of depot steroid but is rare after a well-placed posterior sub-Tenon injection. Often a patient with corticosteroid-induced glaucoma requires maximum medical therapy for both the elevated IOP and the inflammation, and the clinician must prescribe other anti-inflammatory drugs such as NSAIDS.
Surgical Procedures in Secondary Glaucoma and Inflammatory Glaucoma
The preferred procedure for iris bombé may become surgical iridectomy if the media will not allow for laser iridotomy, done with yttrium aluminum garnet (YAG) or argon lasers, because transfixation of the iris or laser iridotomy is often followed by rapid occlusion of the small openings. A surgical iridectomy to treat iris bombé is recommended especially in darkly pigmented eyes (iris) owing to the high risk of immediate iridectomy closure. At the same time, a sub-Tenon capsule injection of corticosteroids may be given.
The results of filtering surgery often are not good. For this surgery, the eye should be as quiet as possible with minimal inflammation. Although laser trabeculoplasty may be tried (if the angle is open), results have not been encouraging,8, 9 and surgical intervention is usually required later. Standard trabeculectomy or other filtering procedures such as modified goniotomy, thermal sclerostomy, and posterior lip sclerotomy have afforded limited success.10, 11 and 12
If the eye has been quiet for several months, however, a standard trabeculectomy filtering procedure has a greater chance of success than when the eye has been quiet for a shorter time. The use of perioperative 5-fluorouracil subconjunctival injections or the intraoperative application of mitomycin C to the episcleral bed has been shown to be beneficial for trabeculectomy success rates.
The surgical strategy that has become popular when facing a progressive secondary glaucoma in uveitic eyes is the use of tube shunt valves or glaucoma drainage devices (GDD). The principles that have made implants successful include the use of a biologically inert silicon tube placed in the anterior chamber (Fig. 64.2) that drains aqueous far from the limbus to an equatorial silicone plate that is sutured to the episclera. What makes this uniquely suited for the benefit of inflammatory glaucoma is the simple fact that the artificial material of the tube is nearly incapable of scarring down the way a naturally fashioned surgical filter would. The variable surface area of this plate allows for the elaboration of a fibrotic bleb across from which there is absorption of the accumulated aqueous.
The Ahmed (New World Medical, Inc.), Baerveldt (Abbott Medical Optics, Inc.), or Molteno (IOP Ophthalmics Inc.) GDD are the more commonly used valves. The Ahmed GDD has the unique ability to immediately control IOP in eyes not responsive to medical therapy due to a valve mechanism built into the plate of the device. The Baerveldt GDD and Molteno GDD must be occluded for approximately 6 weeks before properly functioning. These valves are not without complications. The silicone tube of the GDD may clog with inflammatory debris13, 14, 15 and 16 and irrigation/revision of the GDD and tube may be necessary.
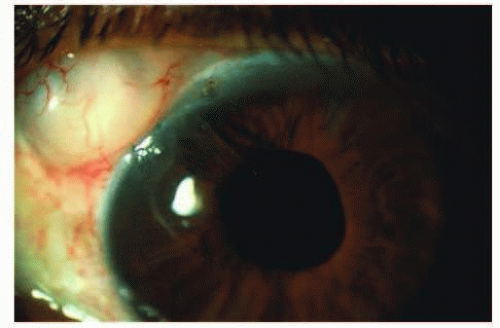
FIG. 64.2 A slit-lamp view of two successive Molteno implants in a 34-year-old patient with Vogt-Koyanagi-Harada disease, who required the second surgery when the first tube clotted with intense fibrous reaction in and around it consequent to profound iridocyclitis.
If both filtering surgery and maximal medical therapy have failed, either cyclocryotherapy or diode transscleral cyclophotocoagulation (CPC) is recommended. Unfortunately, these procedures cause significant inflammation and a definite risk of phthisis bulbi (increasing with each repeated application). Thus, it is a procedure of last resort most commonly performed in eyes with limited visual potential.
Cyclocryotherapy can be performed in a number of ways. The glaucoma cryoprobe can be used with local anesthesia. The inferior 180° of the eye is treated with two rows of freeze for 1 minute at -80°C in three spots per quadrant. The first row begins 2 to 3 mm behind the limbus, with the “ice ball” extending partially onto the cornea. The second row is placed immediately behind the first. By freezing two separate rows, the need to freeze and then refreeze is eliminated. The eye is patched after the instillation of a combined corticosteroid and antibiotic together with a cycloplegic such as atropine 1%. Because patients experience significant pain in the postoperative period, an effective analgesic is important.
CPC with a diode probe is preferred to cyclocryotherapy owing to less inflammation endured by ocular tissues. Retrobulbar or general anesthesia is required for this procedure. The diode probe is configured to the contour of the eye with the steep edge placed just posterior to the corneal limbus. Application regimens are variable. Treatment techniques include placing 12 spots 180?? inferiorly or can be performed 360?? when severely elevated pressure is present. Care is taken to avoid the 3- and 9-o’ clock positions of the eye. The duration of treatment ranges from 1.5 to 2 seconds. As with cyclocryotherapy, a steroid drop, cycloplegic drop, or ointment and patch should be placed.
CATARACT EXTRACTION IN PATIENTS WITH UVEITIS
Cataract formation is a frequent complication of both acute and chronic uveitis. Cataract extractions pose significant risks for patients with uveitis.17, 18, 19, 20 and 21 The outcome of such surgery often depends on the particular uveitis syndrome. Approximately 50% of patients with juvenile rheumatoid arthritis,22, 23 and 24 pars planitis,21 and Fuchs heterochromic iridocyclitis20, 25, 26, 27 and 28 develop visually significant cataracts. Cataract development in patients with uveitis may be a consequence of the inflammatory process or may be iatrogenic as a sequela of corticosteroid therapy. Chronic recurrent uveitis induces cataracts much more frequently than do acute episodes of short duration. Before the advent of corticosteroids in the 1960s, ocular inflammation was difficult if not impossible to control. Cataract surgery was often associated with profound complications both intraoperatively and postoperatively, including retinal detachment, choroidal detachment, vitreous loss, and intraocular hemorrhage. Postoperative complications included severe exacerbations of the intercurrent inflammation with pupillary membrane formation, ciliary body detachment with eventual phthisis, and secondary glaucoma.
The first step in the evaluation of the patients with uveitis for cataract surgery is the accurate classification of the specific disease entity causing the uveitis, the intraocular structures involved, the activity of the inflammation, and a plan for surgery that considers all of the three foregoing factors. These factors and the mode of treatment determine the potential postoperative complications and prognosis of the patient and dictate whether the surgery should be by way of the anterior segment, pars plana, or include the use of an IOL and its type.
Cataract extraction poses significant risks for patients with uveitis. The less inflamed the eye at the time of surgery, the better the prognosis and the less chance of severe postoperative complications.17, 18, 19, 20 and 21, 24, 26, 29 Treating inflamed eyes with high doses of corticosteroids systemically, topically, or by sub-Tenon capsule injection for a few days or a week before surgery is recommended. If posterior inflammation threatens the outcome, such as in recurrent retinal vasculitis, it is wise to defer surgery until the inflammation subsides either naturally or with medication. The advent of small incision phacoemulsification has lessened the intensity of postoperative inflammation, and the use of iris hooks or Malyugin ring to enlarge the pupil has facilitated cataract surgery in patients with chronic uveitis.
The indications for cataract extraction in patients with ocular inflammation are visual disability, maturity of the cataract, and lens-induced inflammation. The necessity to monitor posterior disease (e.g., toxoplasmosis, Vogt-Koyanagi-Harada syndrome, sarcoid, vasculitis, and cystoid macular edema) may also be considered an indication for cataract removal. If the eye has been quiet without medications and there has been no active inflammation for at least several months, a routine lens extraction can usually be performed without significant risk. But when inflammation (even low-grade) is present, special precautions and surgical techniques are necessary.30, 31
If the cataract is mature and there is significant capsular involvement or liquefaction of cortical material, extraction is advisable to prevent lens-induced disorders from being superimposed on an underlying inflammatory process.
The only urgent indication for cataract surgery is the uveitis that appears to have been caused by the lens material itself. Phacoanaphylaxis, phacolytic glaucoma with cataract, and phacotoxic reactions caused by residual lens material after extracapsular lens extractions indicate that the lens or lens material should be removed to eliminate the cause of the active inflammation. If all of the lens material is not removed (both nuclear fragments and cortex), the inflammation may persist indefinitely.
The use of IOL implants is controversial in patients with uveitis.19 All types of IOL compositions and surfaces have been tried, including heparin-coated lenses, to reduce the postoperative accumulation of inflammatory debris and fibrosis coating the new lens.30, 31, 32, 33, 34, 35, 36, 37 and 38 Even transsclerally fixated IOL implants have been attempted in children.39 In general, the condition of the eye and the IOL depends not on which type of IOL implant to instill, but rather the intensity of the ocular inflammation in the postoperative period.33 It is felt that “foldable IOL implantation is safe in uveitic eyes,”34 but that the IOL implant biocompatibility is inversely related to the degree of inflammation present.18, 19, 29, 40 The foldable acrylic IOL implants may be preferred because these patients may have a higher potential for traction/rhegmatogenous retinal detachment on an inflammatory basis, and therefore may have to receive intraocular silicone oil.40, 41 The role of which type of lens composition or surface that leads to or stimulates inflammation the least is still not concluded. Instances of IOL opacification worse than the original cataract are observed and reported.30 However, even series of patients with profound inflammatory basis are noted to do well after cataract surgery if their inflammatory response can be well controlled.30, 33 IOLs have been shown to be tolerated in young patients with juvenile rheumatoid arthritis.35, 42 It still may prevail that even after successful cataract surgery, the vision may not improve satisfactorily because of inflammatory destruction of the retinal structures33 not appreciated before, during, or after the surgery.
Specific Uveitic Syndromes
Juvenile Rheumatoid Arthritis and Iridocyclitis
Early results of extracapsular cataract extraction in patients with juvenile rheumatoid arthritis were not encouraging because of frequent vitreous loss and incarcerations in the cataract wound, development of cyclic membranes, and subsequent ciliary body detachment with eventual phthisis. One report of 15 cases, in which standard extracapsular techniques were used (e.g., aspiration), cited 11 patients with no light perception by the end of 5 years.43
A more encouraging report came from the Proctor Foundation in San Francisco: vision of 20/40 (6/12)* or better was achieved in 60% of patients.24 In the larger series in the literature, Kanski and Shan-Shin27 reported 162 eyes undergoing cataract extraction. The major complication reported in the needle aspiration group was phthisis, and results were improved when lensectomy-vitrectomy was performed. Much more encouraging results have been reported by other investigators after lensectomy-vitrectomy. With lensectomy-vitrectomy surgery, capsule remnants, cyclic membranes, and calcified particles can be removed more completely, thus significantly lessening the possible outcome of ciliary body detachment and phthisis.
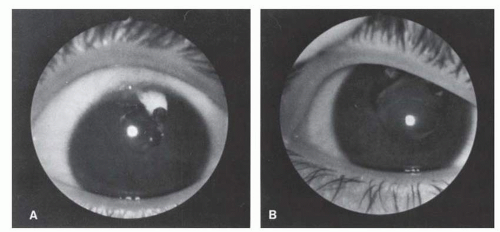
FIG. 64.3 A 16-year-old aphakic white girl with juvenile rheumatoid arthritis. A: Updrawn, fibrotic pupil, with dense cyclitic membrane in a hypotonus eye. B: After pupilloplasty and membranectomy-vitrectomy, a large, round pupil is restored, along with normal ocular tension. Vision improved from counting fingers to 20/40+ (6/12+) with contact lens.
If patients with juvenile rheumatoid arthritis have progressive cataracts and extraction of the lens is indicated, combined lensectomy and subtotal vitrectomy performed through the limbus or pars plana is recommended (Fig. 64.3). An anterior approach for cataract extraction is recommended only when few vitreous opacities are present and the IOP is normal. If there is any suspicion of cyclic membrane with traction on the ciliary body, the treatment of choice is the posterior approach, with vitreous removal to lessen subsequent traction on the ciliary body. This may be suggested by the presence of vitreitis, vitreous opacities, severe anterior segment damage, hypotony, and an obvious cyclic membrane formation. It should be emphasized that meticulous postoperative therapy to prevent amblyopia is equally important as the surgery for full visual rehabilitation in these young patients.
Fuchs Heterochromic Iridocyclitis
Although early reports indicate that bleeding throughout normal angle vessels was a serious complication after cataract extraction in patients with Fuchs heterochromic iridocyclitis,25, 26, 44 this was not proven to be a consistent complication in any of the 29 cases reviewed by Smith and O’Connor.36 Results from the Mayo Clinic have, however, suggested a slight increase in complications after routine cataract extraction in patients with Fuchs iridocyclitis.25 In general, however, any standard procedure for cataract surgery can usually be used without significant risk of intraoperative or postoperative complications. Transient postoperative hyphemas may occur, but seldom create a long-term problem. Because Fuchs iridocyclitis is usually unilateral, the usual indications for this type of cataract extraction apply. The patient’s vision may not return to 20/20 (6/6), however, because the disease itself can cause visually impairing vitreous opacities.
Fuchs heterochromic iridocyclitis is a low-grade, chronic, often asymptomatic anterior uveitis occurring in patients older than 40 years of age. Nearly 100% of patients develop cataracts, usually of the posterior subcapsular type, which is one of the diagnostic features of this disease. Patients with visually significant cataracts as a result of Fuchs syndrome require relatively few special precautions and have a good prognosis after modern extracapsular cataract extraction. The favorable prognosis for successful surgery in these patients may be because of the rarity of posterior synechiae. This is the one uveitic syndrome in which active inflammation may be present and posterior chamber lens implantation (“in the bag”) appears to be well-tolerated with few complications. Gee and Tabbara20 reported postoperative visual acuities of 20/40 or better in all 10 of their patients with Fuchs heterochromic iridocyclitis undergoing extracapsular cataract extraction and posterior chamber lens implantation. The most frequently encountered postoperative complications included hyphema, vitreous hemorrhage, glaucoma, and progression to vitreous opacification, the latter two features being major causes of postoperative visual acuity less than 20/40 as well as being a diagnostic feature of the disease.20, 25
Only gold members can continue reading. Log In or Register to continue