Uveitis in Children
Phoebe Lin
Debra A. Goldstein
Kannan M. Narayana
Levent M. Civelek
Howard H. Tessler
The prevalence of uveitis in children is estimated at approximately 30 in 100,000,1,2 with uveitis accounting for a significant proportion of ocular morbidity in the pediatric population. Children comprise 5% to 20% of cases referred to uveitis clinics in the United States and Great Britain.3,4,5,6,7,8 According to a review by Tugal-Tutkun et al., uveitis may result in blindness in a larger percentage of children than adults with uveitis.9 This may be due to higher rates of severe chronic anterior uveitis and posterior uveitis in children,6,8,10 reinforcing the importance of keeping a low threshold for regular screening in potentially affected patients, and performing a thorough dilated fundus exam despite its relative difficulty in young children. Because early diagnosis and timely treatment can lessen the severity of the disease as well as prevent potentially irreversible complications such as visual loss,11,12 it is important for ophthalmologists and other clinicians to recognize the types of uveitis common in children and the management options that are most appropriate for this age group.
The unique challenges of treating children with uveitis stem from a number of factors. Cunningham eloquently summarized these factors to include (1) delayed diagnosis due to a child’s inability to adequately verbalize symptoms; (2) unique presentations of disease, such as anterior uveitis presenting without the typical symptoms of pain, redness, or photophobia, or sarcoidosis presenting in the skin and joint rather than the lung; (3) difficulty with the examination; (4) different diagnoses that are specific to a younger population; and (5) differences in the physiologically normal range of laboratory values found in children.13 For example, examination under anesthesia may be required in poorly cooperative young patients. Adherence with topical therapy and cooperation during periocular steroid injections may also pose a challenge in treating children. An example in which the physiologically normal range of a laboratory value is different in children than in adults is angiotensin-converting enzyme (ACE) levels, which are physiologically higher in children than in adults on average.14,15,16 Adherence with topical therapy and cooperation during periocular steroid injections may also pose a challenge in treating children. Finally, concomitant with the trials of treating children is the matter of managing parental anxiety and/or parental understanding of the child’s disease, especially for children who are either preverbal or who have minimal physical complaints.
Certain complications of uveitis are more frequent and others perhaps more devastating in the pediatric population. For example, the development of amblyopia due to cataract or dense inflammatory vitreous opacities is unique to childhood.11,17 Severe band keratopathy (Fig. 1) more commonly develops in children than in adults4,18 and can also result in vision loss or amblyopia if it impinges upon the visual axis in younger children. Corticosteroids used to control uveitis can have severe effects on the growth of children by potentially causing premature closure of the epiphyseal plates and thinning or softening of the bones.19,20 Secondary glaucoma is more common in children with uveitis than in adults, due to both corticosteroid use and the inflammatory process itself.21,22,23,24 As with adult uveitis patients, cataract formation is a complication of both chronic inflammation and corticosteroid use, and cataract extraction may be necessary. A great deal of debate surrounds the subject of intraocular lens placement after cataract extraction in children. This will be discussed further in later sections.
 Fig. 1. Severe band keratopathy. |
TYPES OF UVEITIS COMMON IN CHILDREN
Generally speaking, patients under the age of 16 are considered pediatric. In the United States and Great Britain, girls account for more pediatric uveitis cases than boys at a rate of 1.3 or 1.5 to 1.4,5,7,8 Table 1 provides a summary of the patterns of uveitis found in children. Anterior uveitis is typically the most common type of uveitis found in children, accounting for 30% to 60% of cases. Posterior uveitis occurs at a prevalence of 20% to 50%, while intermediate uveitis constitutes about 20%.4,6,7,8,9,11,25,26,27,28,29
TABLE 1. Location and Etiology of Pediatric Uveitis | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Despite advances in diagnostic technology over the past four decades, the etiology and/or syndrome category of up to 54% of childhood uveitis cases remains idiopathic.4,6,7,11,28,29 Common syndrome associations of noninfectious anterior uveitis in children are juvenile idiopathic arthritis (JIA)-associated uveitis and traumatic uveitis.8,9 Toxoplasmosis is the most frequent infectious cause and the most common known etiology of posterior uveitis in children,4,25,28,30 whereas the most common causes of infectious anterior uveitis include herpes simplex and varicella zoster.5 However, rates of toxoplasmosis appear to be decreasing in developed countries over the past four decades.7 The vast majority of intermediate uveitis cases remain idiopathic.9 Less common, yet important, causes of uveitis in children will also be reviewed here, including HLA-B27–associated ocular inflammation (with or without systemic disease), sarcoidosis, Vogt-Koyanagi-Harada disease, sympathetic ophthalmia, Kawasaki disease, toxocariasis, and the tubulointerstitial nephritis and uveitis syndrome. It is also important to recognize the infrequent masquerade syndromes including leukemia, retinoblastoma, retinitis pigmentosa, Coats disease, and juvenile xanthogranuloma.
CLINICAL FEATURES
The presentation of a child with uveitis depends upon the anatomical location of the inflammation. Acute anterior uveitis usually presents with pain, redness, photophobia, and tearing, whereas chronic anterior uveitis is often asymptomatic. It is important for parents and primary clinicians to realize that the initial presenting sign of chronic disease may be merely an irregular pupil (Fig. 2) or failing a school-vision screening test. On ophthalmological examination, signs of anterior uveitis include keratic precipitates (Fig. 3), aqueous cell and flare, iris nodules, iris atrophy, iris neovascularisation, anterior and posterior synechiae, anterior vitreous cells, and cataract. Many eyes will appear completely normal externally yet suffer severe damage over time. Patients can also present with visual loss secondary to cystoid macular edema (CME), a common complication. Intermediate uveitis usually presents with floaters with or without reduced vision, vitreous haze and cells, cellular clumps (snow balls) and pars plana exudates (snow banking). Patients with posterior uveitis often complain of decreased vision, floaters, or photopsias and have vitreous cells, retinitis, choroiditis, optic neuritis, vasculitis (periarteritis or periphlebitis), optic nerve granulomas, or neovascularisation on examination. Treating pediatric patients involves a vast array of complex diagnostic and management issues. This chapter provides an overview of the uveitic entities found in children, a detailed description of the more common problems, and treatment modalities.
 Fig. 2. Patient with posterior synechiae and a grossly irregular pupil. |
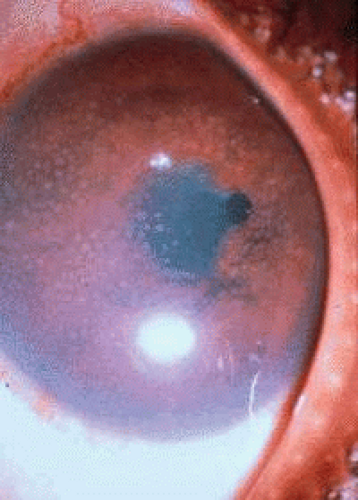 Fig. 3. A child with chronic granulomatous iridocyclitis with multiple keratic precipitates, and an irregular pupil. |
ANTERIOR UVEITIS
Initial Diagnosis of Anterior Uveitis
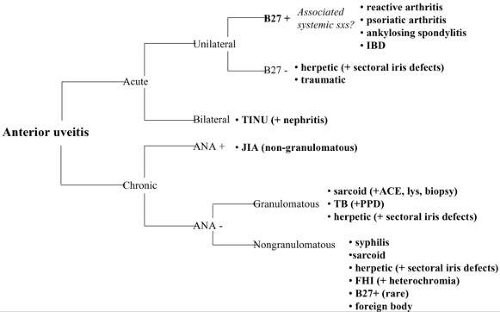
A differential diagnosis for anterior uveitis is developed based on whether the patient has chronic or acute disease, as well as the the presence of other signs, and the results of supplemental laboratory or radiological tests (Table 2). Routine studies that are ordered in both acute and chronic anterior uveitis include a chest x-ray, serum ACE, serum lyzozyme, and a fluorescent treponemal antibody absorption test (FTA-ABS) or a specific treponemal test. Chest x-rays are more commonly normal in children than adults with sarcoidosis, due to the decreased prevalence of pulmonary involvment in the pediatric age group. Skin and joint findings may be the only clues that a child is suffering from sarcoidosis. As in adults, HLA-B27 is one of the more common causes of acute anterior uveitis, and this test is therefore obtained in patients with acute anterior uveitis, regardless of age. In chronic anterior uveitis, antinuclear antibody (ANA) results should be obtained due to a high suspicion for JIA. Other investigations are tailored based on history, review of systems and any other findings on systemic and ocular examination. Aggressive use of corticosteroid topical eye drops along with cycloplegic agents to prevent synechiae formation is usually warranted and continues to form the basis of initial therapy. This is supplemented with immunosuppressive agents and surgery for complications of inflammatory eye disease. The following section describes common anterior uveitic entities in children.
 |
JIA-Associated Uveitis
JIA and Uveitis.
JIA as been recently redefined as any arthritis of unknown etiology lasting for at least 6 weeks beginning before the age of 16.31,32 In the United States, the term juvenile rheumatoid arthritis was used previously, and in Europe, juvenile chronic arthritis was preferred. The most common extra-articular manifestation of JIA is chronic iritis, and any child with chronic anterior uveitis should be suspected of having JIA even in the absence of joint symptoms. The onset of JIA-associated uveitis is often insidious, resulting in a lack of eye complaints and delayed diagnosis. As witnessed from the frequent discovery of myopia on school vision screenings, children seldom complain of blurred vision.
JIA is classified into seven subgroups: (1) systemic arthritis (Still’s disease), (2) oligoarthritis (pauciarthritis), (3) rheumatoid factor–negative polyarthritis, (4) rheumatoid factor–positive polyarthritis, (5) psoriatic arthritis, (6) enthesitis-related arthritis, and (7) other forms of arthritis. Enthesitis-related, psoriatic, and other forms of arthritis are discussed in the section on HLA-B27 disease. Pauciarticular JIA is defined as having 1 to 4 joints affected during the first 6 months of disease, typically involving the knees,32 although sometimes only affecting a single toe or finger.33 Oligoarthritis is 3 to 4 times more common in girls than in boys, with a peak age of onset between 2 and 4 years of age. Polyarthritis affects five or more joints and involves both large and small joints in children of any age.32 Oligoarticular disease and younger age at onset appear to be independent risk factors for the development of uveitis.32,33
While uveitis rarely occurs in systemic arthritis and rheumatoid factor–positive polyarthritis, it occurs in up to 20% of patients with the oligoarthritis or pauciarticular form of JIA.33,34 Uveitis is especially prevelant in those who are ANA positive and have early-onset oligoarthritis.32,35,36 In one series, ANA was positive in 71% to 93% of patients with uveitis compared to 30% of JIA patients without eye involvement.37 A small subgroup of patients have also been described who are ANA positive with chronic iridocyclitis reminiscent of JIA-associated uveitis who do not have arthritis.32 These patients may correspond to a subgroup that develops uveitis prior to the development of JIA, or who have JIA-like uveitis without joint manifestations. It is also possible that some of these children had mild pauciarticular arthritis that resolved without diagnosis.
Uveitis occurs in 5% to 10% of patients with rheumatoid factor–negative polyarthritis33,34 and can also be associated with psoriatic arthritis, although prevalences are not discussed in the literature, as the latter is a relatively rare entity in the pediatric population.
In the majority of cases, uveitis follows the onset of arthritis. However, it is often the case that the main problem for the patient is the uveitis while the arthritis resolves or undergoes complete remission. Ninety percent of the time, uveitis is diagnosed within 7 years of JIA diagnosis.32,33 On the other hand, uveitis precedes arthritic symptoms in up to 10% of cases. A longer interval from the onset of arthritis symptoms to the diagnosis of uveitis has been associated with a reduced risk of severe uveitis at diagnosis.38
Presentation and Screening.
JIA-associated uveitis is typically chronic, insidious, and nongranulomatous. It is bilateral in 75% to 89% of cases.25,26,33,39,40 Both eyes tend to be affected simultaneously or within a few months of each other, although the inflammation is often asymmetric. Keratic precipitates are usually located on the lower half of the cornea and are small to medium in size.33 Arthritic flare-ups do not correlate with the severity of uveitis, emphasizing the importance of regular slit lamp biomicroscopic screening in all JIA patients, regardless of severity of arthritis. Indicators for a better prognosis include male sex, good visual acuity at presentation, diagnosis of uveitis after the onset of joint disease, and onset of disease at an older age.41 Screening recommendations for patients with JIA are shown in Table 3.33,40
TABLE 3. Screening Recommendations for JIA-Associated Uveitis | |
|---|---|
|
Pathophysiology.
The etiology of JIA is unknown. Pathologic specimens, usually from late-stage disease, demonstrate nonspecific infiltration of the iris and ciliary body with lymphocytes and plasma cells.42 The strongest correlation with JIA-associated uveitis is the presence of ANA. However, this is also a relatively nonspecific marker for autoimmune disease. Clues as to the pathogenesis of JIA-associated uveitis may ultimately be found by looking at differences in the immunological response in systemic JIA, in which uveitis rarely occurs, in contrast to oligoarticular JIA, in which a relatively large proportion develop uveitis. Studies have shown that while interleukin-6 (IL-6) expression and a primarily Th1-type lymphocyte response occurs in systemic JIA, a predominance of suppressor T cells with IL-4 and IL-10 production occurs in oligoarticular JIA.43 Certain genetic markers have been attributed to JIA patients who develop uveitis, perhaps increasing their susceptibility to develop disease. For instance, HLA-DR5 and HLA-DPw2 have been associated with oligoarticular JIA and uveitis, whereas patients who express HLA-DR1 and HLA-DR4 are less likely to develop uveitis.44,45,46,47 In one study, over 70% of patients with JIA-associated uveitis were positive for HLA-DR5, representing a significantly higher number than the control group.44
Management.
Early and aggressive treatment is imperative in JIA-associated uveitis and has been shown to reduce irreversible vision-threatening complications.12,40 Patients are usually started on topical steroids at a rate of 1 to 4 times a day and, rarely, as frequently as every hour (Table 4). There may be great difficulty in administering frequent drops to young children. It is a burden on the parents and the child, and more frequent drops increase the risk of cataract development. Mydriatics such as cyclopentolate, homatropine, or tropicamide are used weekly to as often as 1 to 3 times a day, depending on the severity of inflammation.32 The latter are used in order to prevent posterior synechiae formation. Atropine may be necessary for severe cases, or in the unreliable patient. However, atropine should not be overused, as constant cycloplegia can induce ambylopia in young children, and young children are more succeptible to anticholinergic toxicity than are adults.33
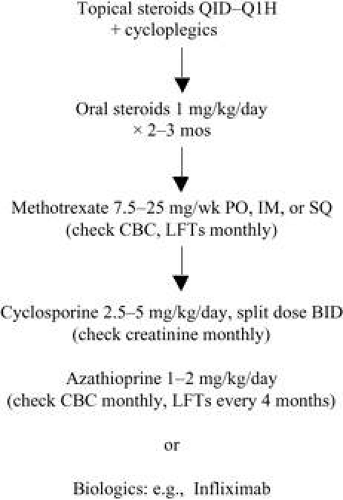 |
If the uveitis is refractory to topical treatment or requires very frequent drops to control, systemic therapy may be added. Some studies suggest that adding systemic nonsteroidal anti-inflammatory drugs (NSAIDs) can reduce inflammation and allow for tapering of steroids.38,48 We have found that when NSAIDs are reduced on improvement of arthritic symptoms, ocular inflammation may flare. Systemic corticosteroids may be used, and are typically started at 1 mg/kg/day. However, due to their vast array of potential side effects including severe growth retardation in children,20 high-dose systemic corticosteroids should be used only for brief periods (2 to 3 months) and should be tapered off by 3 to 4 months. Children less than 15 years of age may have a delay in pubertal growth even when prednisone therapy is used every other day.49
If oral corticosteroid therapy is required for more than 2 to 3 months, steroid-sparing agents are recommended. Methotrexate has been shown to be safe and effective in children with severe JIA-associated uveitis.50,51 It is usually given at a dose of 7.5 to 25 mg/week either orally, intramuscularly, or subcutaneously (Table 4).32 Because of its relative safety in children, methotrexate is often used as a first-line agent over systemic steroids. Common side effects of methotrexate include nausea, vomiting, and oral stomatitis. Hepatotoxicity and cytopenia can can also occur. Liver function tests and complete blood counts are evaluated before initiation of therapy and should be monitored every 1 to 2 months thereafter. The dose of methotrexate should be reduced if the aspartate aminotransferase or alanine aminotransferase level is more than twice normal on two separate occasions.52 In our practice, any elevation above the normal limit is an indication for dose reduction. A liver biopsy may be warranted if liver enzymes remain elevated after the drug is discontinued.
If uveitis is active despite the use of systemic steroids and/or methotrexate, immunomodulatory drugs may be added, including cyclosporine, used at 2.5 to 5 mg/kg/day administered as equally divided twice daily oral doses. Azathioprine given orally at a dose of 1 to 2 mg/kg/day is substituted if methotrexate is not tolerated.53,54,55,56,57 Cyclosporine can cause nephrotoxicity, hypertension, hepatotoxicity, gingival hyperplasia, hypomagnesemia, and hirsutism.57,58 Screening for patients taking cyclosporine should include blood pressure checks no less than monthly initially and then every 3 months thereafter, as well as a serum creatinine test every 2 weeks in the beginning of therapy, and then monthly once the dosage is established.52 The most common side effect of azathioprine is gastrointestinal intolerance, although more severe side effects include bone marrow suppression and hepatotoxicity. Treatment with this immunomodulator requires regular screening of complete blood counts every 4 to 6 weeks and liver function tests every 12 weeks. If liver functions tests are greater than 1.5 times the upper limit of normal, the dose should be reduced by 25 to 50 mg/day, and liver function tests repeated in 2 weeks. If liver function tests are elevated greater than five times the upper limit of normal, one should discontinue the drug pending a return to normal in liver enzymes.52
Alkylating agents such as chlorambucil and cyclophosphamide are seldom used for JIA-associated uveitis except for the most severe cases, due to their numerous risks and toxicity. These include sterility and bone marrow suppression for chlorambucil. Cyclophosphamide also causes bone marrow suppression as well as hemorrhagic cystitis and gonadal failure. There is also an increased risk of bladder cancer with cyclophosphamide use.40,52 Both drugs are teratogenic and increase the lifetime risk of developing cancer.
New options for the treatment of JIA-associated uveitis include the use of disease-modifying drugs such as the tumor necrosis factor-alpha antagonist biologics infliximab and etanercept. These drugs are being utilized more and more often for the treatment of refractory autoimmune arthritic and dermatologic conditions in both adults and children. While some studies report good long-term outcomes in pediatric patients with JIA-associated uveitis who were treated with etanercept,59 other studies do not show any benefit compared with placebo.60 A large survey of pediatric rheumatologists reported no decrease in uveitis recurrences in JIA patients treated with etanercept for their joints. In fact, many patients had their first attack of uveits while on etanercept.61 Infliximab now appears to be emerging as a much more effective treatment than etanercept in the treatment of uveitis.62 Long-term effects of these drugs on children and adults are controversial regarding a potentially increased, albeit low, risk for cancer.
Complications.
A large percentage (up to 75%) of children with moderate to severe uveitis suffer from significant visual loss due to ocular complications.63,64,65 Cataract is a common complication (Fig. 4) occurring in 21% to as high as 84% of JIA patients with uveitis.8,11,35,38 Cataract in uveitis patients may develop because of anterior chamber inflammation and corticosteroid use, both of which may result in posterior subcapsular or other type of cataract. Historically, patients with pediatric chronic iridocyclitis have done poorly with cataract surgery. The outcome of cataract extraction has improved recently with emphasis on strict perioperative control of inflammation and newer surgical techniques. In fact, the majority of children with JIA-associated uveitis who undergo cataract extraction attain postoperative visual acuity of 20/40 or better.66,67
 Fig. 4. Juvenile idiopathic arthritis patient with cataract and band keratopathy. Note the laser peripheral iridotomyThis patient has 360° of posterior synechiae. |
Intraocular lens implantation in children with uveitic cataract is a controversial issue because of potentially higher rates of complications, especially in younger children. These include posterior lens capsule opacifications and formation of membranes enveloping the intraocular lens (i.e., cocooning), both of which can lead to amblyopia.67,68,69 Cocooning membranes can also cause traction on the ciliary body, ultimately resulting in hypotony and phthisis. Because of these complications, pediatric patients were, in the past, left aphakic after cataract extraction. Lensectomy-vitrectomy was the recommended therapy to help prevent pupillary membrane formation, hypotony, and phthisis. Aphakia was subsequently corrected with glasses or contact lenses. However, poor contact lens compliance and the subsequent development of amblyopia in younger children were typical problems. Now, it is felt by some authors that posterior chamber intraocular lens implantation, usually with posterior capsulorhexis and anterior vitrectomy, can be safely considered for JIA patients who develop cataract,67 although this is still controversial. Some physicians prefer to reserve implantation for older JIA patients who have not had active inflammation for a number of years. It is imperative to control inflammation perioperatively by making sure the eye is quiescent for 3 to 4 months before cataract surgery, with continuing aggressive inflammation control postoperatively. If the inflammation is not well controlled or if the patient cannot be relied upon to diligently comply with the medication regimen, an intraocular lens should not be placed.
Secondary glaucoma occurs in 8% to 37% of patients with JIA-associated uveitis and can be due to inflammation or as a result of corticosteroid use.8,24,32,35,38,70,71 Elevation of intraocular pressure often arises as inflammation subsides, because aqueous secretion improves without adequate recovery of outflow capacity after chronic inflammatory damage has occurred.24 Glaucoma in this setting is often refractory to standard medical treatment with topical beta-blockers and topical or systemic carbonic anhydrase inhibitors. The prostaglandins were avoided in the past because of reports that they caused uveitis.72 However, many clinicians believe that prostaglandin analogs are relatively safe in patients with uveitis. The concomitant use of anti-inflammatory therapy may prevent worsening of uveitis in the context of prostaglandin use. Also, if the uveitis is under control, the use of less powerful topical corticosteroids may be of benefit in lowering intraocular pressure. Glaucoma surgery may be required in treating patients with uveitic glaucoma. Surgical techniques that have been effective include filtering surgery with or without antimetabolites and valve drainage procedures.24,73
Band keratopathy is the deposition of calcium hydroxyapatite in Bowman layer of the cornea, often distinctly located in the interpalpebral zone (Fig. 5). It occurs more often in pediatric uveitis patients than in adults and is found in up to 70% of patients with JIA-associated uveitis.38 Development of band keratopathy can result in central corneal opacity and amblyopia in younger children. Irregularities in the band can result in dellen formation, corneal ulcer, and perforation. Chelating agents or excimer lasers have been used to remove the band, but deposition tends to recur.
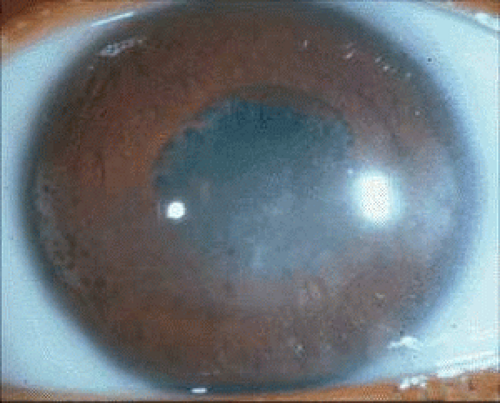 Fig. 5. Patient with juvenile idiopathic arthritis and interpalpebral band keratopathy. Also note the posterior synechiae and irregularly shaped pupil. |
CME, posterior synechiae, retinal detachment, hypotony, and phthisis bulbi are other complications of long-standing inflammation in children. CME occurs secondary to anterior chamber inflammation and may be treated with systemic corticosteroids or local periocular steroid injections. If vision is threatened by CME, immunosuppressives may also be used.12
HLA-B27–Associated Uveitis
HLA-B27 is a class I major histocompatibilty antigen that predisposes patients to certain seronegative autoimmune diseases including ankylosing spondylitis, reactive arthritis (previously known as Reiter’s syndrome), psoriatic arthritis, and inflammatory bowel disease. HLA-B27–associated uveitis comprises approximately 16% of anterior uveitis in children.41
Many pediatric patients with psoriatic- and enthesitis-related forms of JIA and uveitis are positive for HLA-B27. Juvenile ankylosing spondylitis is a syndrome of seronegative enthesopathy and arthopathy, affecting the axial skeleton (e.g., sacroiliitis) in children, most often between 8 and 10 years of age.74,75 Boys are affected more commonly than girls, as with adults. Unlike adults, however, juvenile ankylosing spondylitis frequently presents as a peripheral arthropathy before physical or radiographic findings of sacroiliac joint involvement are seen. Both the adult and juvenile forms are associated with HLA-B27 in over 90% of patients.76,77 Reactive arthritis is a syndrome commonly involving a triad of symptoms including arthritis, urethritis, and conjunctivitis. Uveitis occurs in up to 20% of these patients.78 Reactive arthritis is associated with HLA-B27 in 75% of patients,79 and this is increased further if uveitis is present also.80 Inflammatory bowel disease, comprising ulcerative colitis and Crohn’s disease, is rare in children and is associated with uveitis in 2% to 11% of patients. However, only 50% of inflammatory bowel disease patients are HLA-B27 positive.81
Ocular Presentation and Complications.
HLA-B27–associated uveitis usually occurs in boys over the age of 16. In contrast to JIA-associated uveitis, the HLA-B27–associated form tends to cause nongranulomatous, acute, unilateral anterior uveitis. Recurrences are common, and inflammation may alternate between eyes. Uveitis in this setting typically presents with the symptoms of pain, redness, and photophobia. Fibrin deposition and hypopyon formation may be present. Uveitis can precede or follow arthritis. HLA-B27–associated uveitis can also occur in the absence of joint or enteric symptoms. In general, inflammatory activity is unrelated to arthritic activity.75,82 Complications of HLA-B27–associated uveitis include cataract, glaucoma, and posterior synechiae formation. Juvenile psoriatic arthritis is a rare pediatric disease entity, and is more often associated with chronic rather than acute anterior uveitis.83 Uveitis that is associated with inflammatory bowel disease may present with chronic, bilateral, and posterior pole inflammation, with CME occurring frequently.84,85
Management.
Patients with acute attacks of HLA-B27–associated uveitis are treated with topical corticosteroids and cycloplegics. Severe attacks with hypopyon may require periocular corticosteroid injection or a short course of oral corticosteroids. If the formation of fibrinous membranes threatens to cause pupillary block, intracameral tissue plasminogen activator has been shown to be effective in dissolving membranes and disrupting posterior synechiae, although this is rarely required.86 Because these uveitic episodes are usually self-limited, immunosuppressives are seldom necessary.
Sarcoidosis
Sarcoidosis, characterized by multiorgan infiltration of noncaseating inflammatory granulomas, most commonly presents in the eyes of children as anterior uveitis.87,88,89 Sarcoidosis can involve the lungs, skin, joints, liver, parotid glands, and central nervous system. In children younger than 5 years of age, however, the lungs are less commonly affected, while the joints, skin, and eyes are more likely to be involved.88,89,90,91 The location of sarcoid involvement in children 8 to 15 years of age is similar to that in adults.90 African American children are affected more commonly than Caucasians.92 Additionally, among children 8 to 15 years of age, boys and girls are equally affected. This is in contrast to adults, in whom females are more commonly affected. Sarcoidosis presenting in children under the age of 5 shows a slight preference for girls.92
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


