8 Uveitis
Pathophysiology
Inflammatory reaction
Anterior uveitis
Inflammation of iris (iritis) and ciliary body (cyclitis)
Most common cause of anterior uveitis in adults is idiopathic (followed by HLA-B27 associated)
Most common cause of acute, noninfectious, hypopyon iritis is HLA-B27-associated iritis
Etiology
Classification
Findings
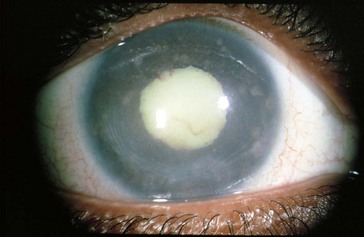
conjunctival and episcleral injection, ciliary injection (circumcorneal flush from branches of anterior ciliary arteries), miosis (iris sphincter spasm), AC reaction; may have hypopyon, keratic precipitates, iris nodules, dilated iris vessels (occasionally, rubeosis), synechiae (posterior [iris adhesions to lens; seclusio pupillae is a complete adhesion that can result in iris bombe] or anterior [iris adhesions to cornea and angle]) (Figure 8-1)

Figure 8-1 Severe idiopathic anterior uveitis with fibrinoid reaction.
(From Hooper PL: Idiopathic and other anterior uveitis. In Yanoff M, Duker JS [eds]: Ophthalmology, London, Mosby, 1999.)
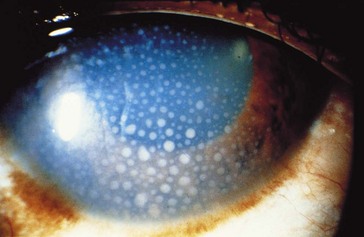
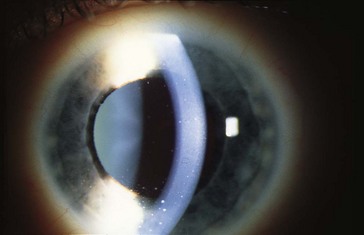
Figure 8-2 Keratic precipitates in anterior uveitis.
(From Forster DJ: General approach to the uveitis patient and treatment strategies. In Yanoff M, Duker JS [eds]: Ophthalmology, London, Mosby, 1999.)
Diagnosis
Treatment
topical steroids, cycloplegic; may require systemic steroids, immunosuppressive agents, antibiotics
Reiter’s Syndrome
Triad of conjunctivitis, urethritis, and arthritis
Associated with infections: Chlamydia, Ureaplasma urealyticum, Yersinia, Shigella, Salmonella
Psoriatic Arthritis
Associated with HLA-B17 and HLA-B27
Uveitis does not occur in psoriasis without arthritis
Inflammatory Bowel Disease (IBD)
Uveitis occurs in ulcerative colitis (10%) and Crohn’s disease (3%)
Fuchs’ Heterochromic Iridocyclitis
Occurs in young adults; unilateral
Associated with chorioretinal scars (toxo)
Findings
diffuse small white stellate KP, minimal AC reaction, no posterior synechiae, iris heterochromia (diffuse atrophy of stroma, loss of iris crypts; involved iris is paler; 15% bilateral), fine-angle vessels (may bleed during gonioscopy, cataract surgery, or paracentesis) (Figure 8-4)
Lyme Disease
Due to Borrelia burgdorferi (spirochete)
Ocular involvement is usually bilateral
Affected organ systems: skin, CNS, cardiovascular, musculoskeletal
Posner-Schlossman Syndrome (Glaucomatocyclitic Crisis)
Recurrent anterior uveitis and increased IOP; episodes are typically self-limited
Phacoanaphylactic Endophthalmitis
May develop severe uveitis with hypotony, secondary open-angle glaucoma
Intermediate uveitis
Pars Planitis
Most common cause of intermediate uveitis (85–90%)
Usually young adults; females > males; 75% bilateral
Accounts for 25% of uveitis in children
Associated with HLA-DR15 and MS
Findings
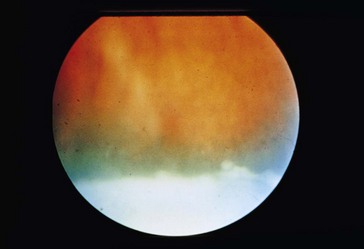
light flare with a few KP, anterior vitritis, snowballs (white vitreous cellular aggregates near ora serrata; may coalesce to form peripheral fibrovascular accumulation [snowbank] over inferior pars plana and vitreous base), peripheral retinal periphlebitis, hyperemic disc, no chorioretinitis, no synechiae (Figure 8-5)
 with exacerbations)
with exacerbations)Posterior uveitis
Most common cause of posterior uveitis in adults is toxoplasmosis (followed by retinal vasculitis)
Infections
Cytomegalovirus (CMV)
Progressive hemorrhagic necrotizing retinitis involving all retinal layers
Occurs in 15–46% of AIDS patients; usually when CD4 count <50 cells/mm3
Rare syndrome of neonatal cytomegalic inclusion disease
Findings
well-circumscribed necrotizing retinitis (2 appearances), mild AC and vitreous reaction
Treatment
antiviral therapy (induction during first 2 weeks)
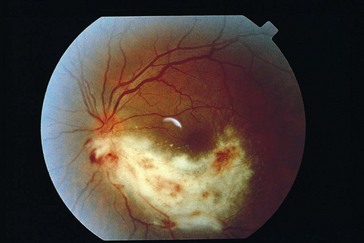
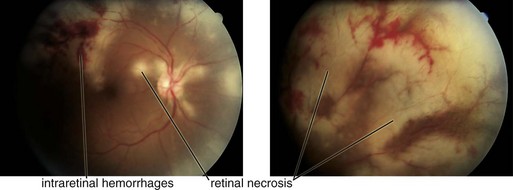
Acute Retinal Necrosis (ARN)
Usually occurs in immunocompetent individuals; 33% bilateral (BARN), commonly in immunosuppressed
Association with HLA-DQw7 (50%)
Findings
diffuse episcleral injection, mild iritis with granulomatous KP, vitritis; ‘thumbprint’ nummular infiltrates posterior to equator with isolated peripheral patches of necrotizing retinitis that becomes confluent; sawtooth demarcation line between necrotic and healthy retina, generalized obliterative retinal arteritis (with peripheral vaso-occlusion), pale disc edema (Figure 8-7); within 2 months, retinitis gradually resolves and necrotic retina sloughs; coarse salt and pepper pigmentation
Progressive Outer Retinal Necrosis (PORN)
Variant of ARN in AIDS but painless with minimal intraocular inflammation
Often have history of cutaneous zoster
74% unilateral at presentation, 70% become bilateral
Findings: multiple discrete peripheral or central areas of retinal opacification/infiltrates (deep with very rapid progression), ‘cracked mud’ appearance after resolution; vasculitis is not prominent (Figure 8-8)

Figure 8-8 Progressive outer retinal necrosis, early stage.
(From Hudson HL, Boyer DS, Martin DF, et al: Viral posterior uveitis. In Yanoff M, Duker JS [eds]: Ophthalmology, London, Mosby, 1999.)
Treatment: combination of foscarnet and ganciclovir; poor response to antivirals



