4 Neuro-ophthalmology
Anatomy of the Visual Pathway
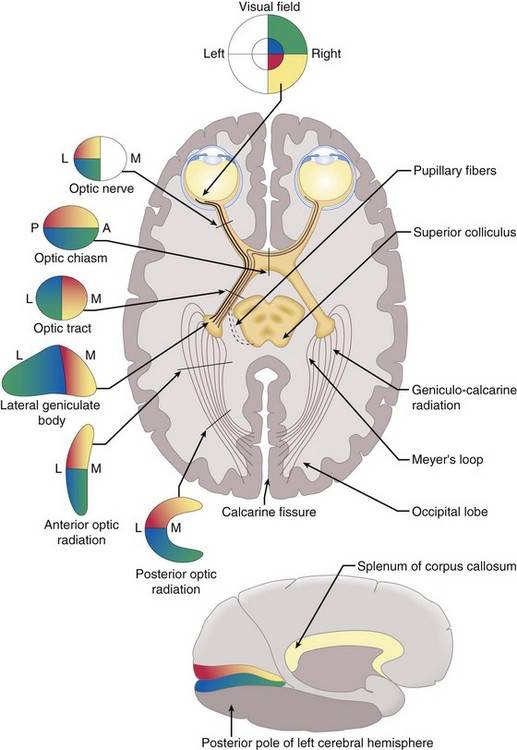
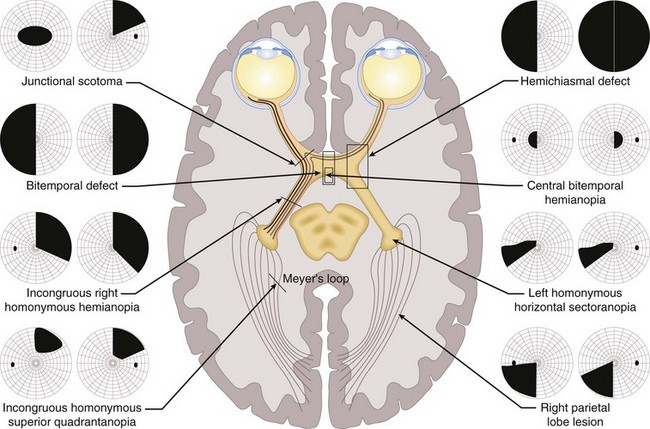
Optic nerve → chiasm → optic tract → lateral geniculate body → optic radiation → occipital lobe (Figure 4-1)
Optic nerve
composed of 1.2 million nerve fibers; approximately 1.5 mm in diameter, enlarges to 3.5 mm posterior to lamina cribrosa due to myelin sheath; located 3–4 mm from fovea; causes absolute scotoma (blind spot) 15° temporal to fixation and slightly below horizontal meridian; approximately 45-50 mm in length (1 mm intraocular, 25 mm intraorbital, 9 mm intracanalicular, 10–15 mm intracranial) (Figure 4-2); acquires myelin posterior to lamina cribosa
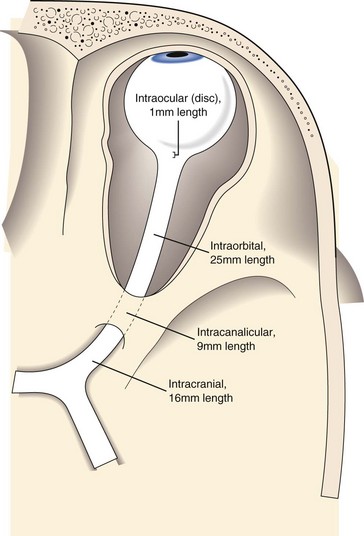
Figure 4-2 The 4 portions of the optic nerve. The lengths are given.
(From Sadun AA: Anatomy and physiology. In: Yanoff M, Duker JS (eds) Ophthalmology, 2nd edn. St Louis, Mosby, 2004.)
Chiasm
Optic tract
Lateral geniculate body
part of the thalamus (Figure 4-5)
Optic radiation
myelinated nerve fibers; connect LGB to occipital cortex
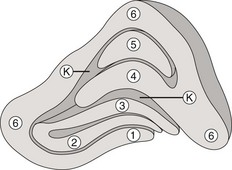
Primary visual cortex (striate cortex, V1, Brodmann’s area 17)
medial face of occipital lobe, divided horizontally by calcarine fissure
Other areas
 of tongue
of tongue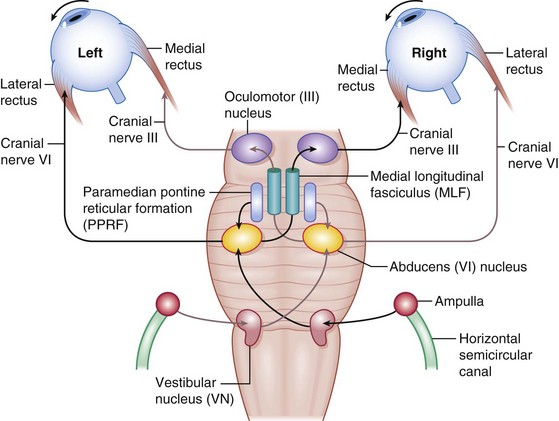
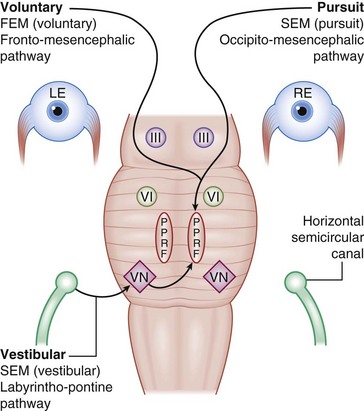
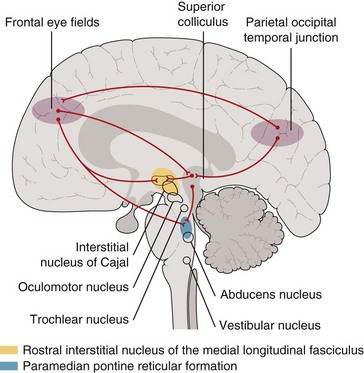
Figure 4-6 Horizontal eye movement pathways.
(From Bajandas FJ, Kline LB: Neuro-Ophthalmology Review Manual. Thorofare, NJ, Slack, 1988.)
Physiology
Testing
Color vision tests
Ishihara pseudoisochromatic or Hardy-Rand-Ritter plates; Farnsworth tests
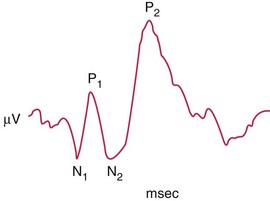
Visually evoked cortical potentials / responses (VEP, VER)
measure macular visual function, integrity of primary and secondary visual cortex, and continuity of optic nerve and tract radiations; fovea has large area in occipital cortex, close to recording electrodes; smaller area representing more peripheral retina lies deep within calcarine fissure (Figure 4-8)
Optokinetic nystagmus (OKN)
presence suggests visual input is present; slow phase is noted in direction of moving stimulus
Can use to diagnose functional visual loss
Visual Field (VF) Defects (Figure 4-9)
Types
Neurologic VF defects
Eye Movements under Supranuclear Control
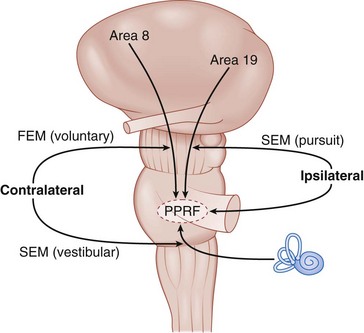
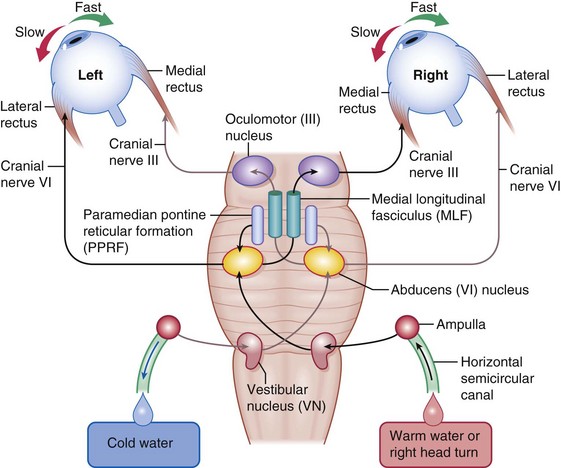
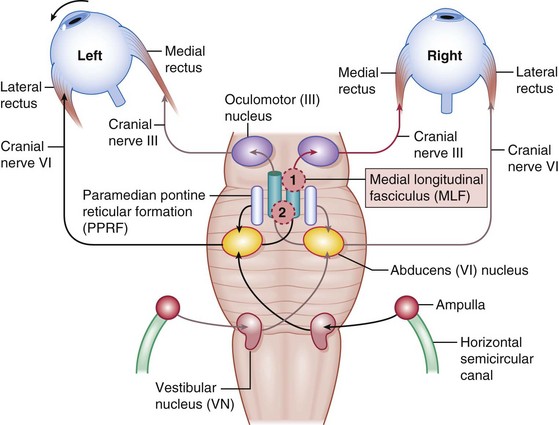
Horizontal gaze center (Figures 4-10,4-11)
Saccadic system
generates fast eye movements (FEM) (refixation); 300-700°/s
Position maintenance system (vestibulo-ocular reflex [VOR])
maintains specific gaze position during head movements
Nonoptic reflex systems
integrate eye movements with body movements
Diplopia
Etiology
Differential diagnosis (DDx)
Eye Movement Disorders
Central Disorders (Supranuclear) (Figure 4-13)
Often no symptoms or complaints
Horizontal Gaze Palsies
Möbius’ Syndrome
Horizontal gaze palsy with CN 6, 7, 8, and 9 palsies (facial diplegia, deafness, abnormal digits)
Ocular Motor Apraxia
Acquired
Pseudogaze palsies
myasthenia gravis, chronic progressive external ophthalmoplegia (CPEO), Duane’s syndrome
Internuclear ophthalmoplegia (INO) (Figure 4-14)
 syndrome may develop oculopalatal myoclonus
syndrome may develop oculopalatal myoclonus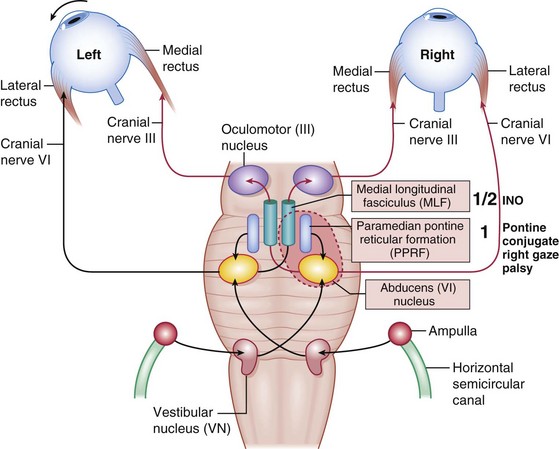
 syndrome (paralytic pontine exotropia).
syndrome (paralytic pontine exotropia).Vertical Gaze Abnormalities
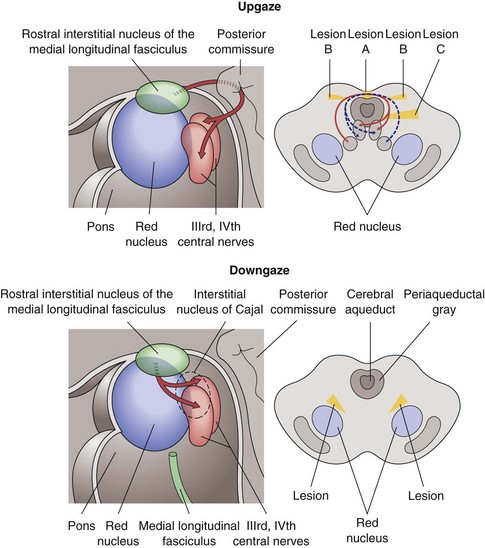
Parinaud’s Syndrome (Dorsal Midbrain Syndrome)
Supranuclear gaze palsy with nuclear CN 3 palsy
Skew Deviation
Vertical misalignment of visual axes due to imbalance of prenuclear inputs; comitant or incomitant
Whipple’s Disease
Oculomasticatory myorhythmia (vertical eye movements and facial activity similar to myoclonus)
Olivopontocerebellar Atrophy
Eye movements progressively slow in all directions, finally complete external ophthalmoplegia
Nystagmus
Childhood Nystagmus
Most commonly, congenital, latent, sensory, and spasmus nutans (see Ch. 5, Pediatrics / Strabismus)
Physiologic Nystagmus
Several forms of nystagmus, including end-gaze, optokinetic, caloric, and rotational
Acquired Nystagmus
Pattern helps localize pathology, may have oscillopsia
Convergence-Retraction
Cocontraction of lateral recti produces convergence movement (abnormal saccades) on attempted upgaze
Dissociated
Asymmetric between the 2 eyes (different direction, amplitude, frequency, etc); always pathologic
Gaze-Evoked
Nystagmus in direction of gaze, absent in primary position, fast phase toward lesion (cerebellar)
If asymmetric, must obtain neuroimaging
Vestibular
Due to vestibular disease, infection (labrynthitis), Ménière’s disease, vascular, trauma, toxicity
Other Eye Movement Disorders
Ocular Bobbing
Intermittent conjugate rapid downward eye movements followed by slow return to primary position
Opsoclonus (Saccadomania)
Rapid, chaotic eye movements in all directions; persists in sleep
Associated with dancing hands and feet
Abnormality of pause cells (normally suppress burst cells of PPRF)
Cranial Nerve Palsies (FIGURE 4-16)
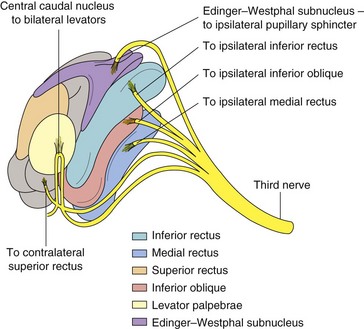
Oculomotor Nerve (CN 3) Palsy
Anatomy
Only 1 subnucleus (midline location) supplies both levator palpebrae superioris; fibers from superior rectus (SR) subnucleus supply contralateral SR; Edinger-Westphal nucleus supplies both pupils (Figure 4-18)
7 syndromes (Figure 4-17)
 ): extremely rare; contralateral SR paresis and bilateral ptosis; pupil involvement is both or neither
): extremely rare; contralateral SR paresis and bilateral ptosis; pupil involvement is both or neither ): ischemic, infiltrative (tumor), or inflammatory (rare)
): ischemic, infiltrative (tumor), or inflammatory (rare) ): supratentorial mass may cause uncal herniation compressing CN 3
): supratentorial mass may cause uncal herniation compressing CN 3 ): most common nontraumatic, isolated, pupil involving CN 3 palsy; aneurysm at junction of PCom and carotid artery compresses nerve, particularly external parasympathetic pupillomotor fibers; usually painful
): most common nontraumatic, isolated, pupil involving CN 3 palsy; aneurysm at junction of PCom and carotid artery compresses nerve, particularly external parasympathetic pupillomotor fibers; usually painful ): associated with multiple CN palsies (3, 4, V1, 6) and Horner’s; CN 3 palsy often partial and pupil sparing; may lead to aberrant regeneration
): associated with multiple CN palsies (3, 4, V1, 6) and Horner’s; CN 3 palsy often partial and pupil sparing; may lead to aberrant regeneration ): tumor, trauma, pseudotumor, or cellulitis; associated with multiple CN palsies (3, 4, V1, 6), proptosis, chemosis, injection; ON can appear normal, swollen, or atrophic
): tumor, trauma, pseudotumor, or cellulitis; associated with multiple CN palsies (3, 4, V1, 6), proptosis, chemosis, injection; ON can appear normal, swollen, or atrophic ): small-caliber parasympathetic pupillomotor fibers travel in outer layers of nerve closer to blood supply (but more susceptible to damage by compression); fibers at core of nerve are compromised by ischemia; may explain pupil sparing in 80% of ischemic CN 3 palsies and pupil involved in 95% of compressive CN 3 palsies (trauma, tumor, aneurysm)
): small-caliber parasympathetic pupillomotor fibers travel in outer layers of nerve closer to blood supply (but more susceptible to damage by compression); fibers at core of nerve are compromised by ischemia; may explain pupil sparing in 80% of ischemic CN 3 palsies and pupil involved in 95% of compressive CN 3 palsies (trauma, tumor, aneurysm)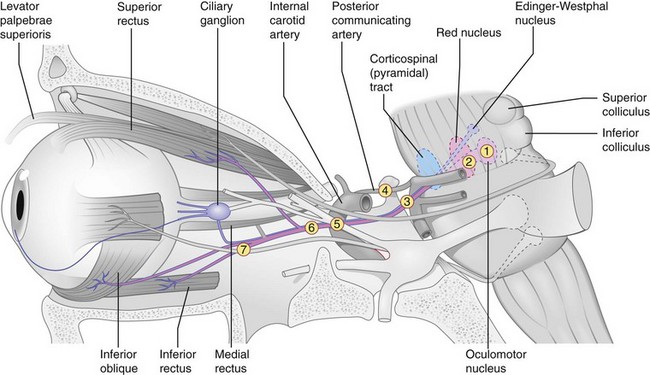
Aberrant regeneration
Other causes of CN 3 palsy
Workup



