Uveal Biopsy
Darius M. Moshfeghi
Gholam A. Peyman
Surgical biopsy is the mainstay of tissue diagnosis in all areas of medicine. When faced clinically with a diagnostic dilemma, the surgeon must carefully choose a biopsy technique to match the desired goals. Various techniques employed include en bloc organ removal (e.g., enucleation), excisional biopsy, incisional biopsy, and fine-needle aspiration biopsy. Biopsy may be required to establish the diagnosis for further therapy or may be therapeutic in itself by en bloc excision of the involved tissue. When clinical clues and laboratory testing are insufficient, often surgical biopsy allows the pathologist to assist in diagnosis. Close collaboration with ocular pathologists and cytopathologists is important to achieve the diagnosis.
In ophthalmic surgery, biopsy has been used in lesions involving adnexal, orbital, anterior, and posterior segment. Surgical specimens of the eyelid and conjunctiva are easily obtained with minimal surgical trauma. Anterior segment lesions are readily accessible, and excisional biopsies of iris lesions are accomplished by open iridectomy.
The more posterior uveal lesions, including those of the ciliary body and choroid, are not as accessible to excisional, incisional, or fine-needle biopsy. Specialized techniques, surgical skill, and experience are often necessary to achieve the desired goals without complications.1,2 One study indicated that in specialized oncology units, 0.5% to 1% of eyes enucleated for suspicious malignant tumors may be nonmalignant on histopathology.3 The percentage may be higher in other centers. Biopsy has a diagnostic role in avoiding unnecessary globe removals. Newer refinements in surgical technique and instrumentation allow skilled ophthalmic surgeons to perform biopsy in posterior uveal lesions.
Posterior uveal biopsy may be achieved by fine-needle aspiration techniques, either under direct visualization or ultrasonographic control.4 Vitreous biopsy may be performed with needle aspiration5 or, preferably, with cutting vitrectomy instruments to reduce the vitreous-retinal traction and risk of retinal detachment. These forms of biopsy provide small biopsy samples without damage to histologic architecture. Large-bore needles have been used to gather cellular cores; however, they also can cause more vascular and tissue trauma. Clinical diagnostic difficulties with amelanotic malignant melanoma, infections,6,7 inflammation,8 and metastatic tumors9,10,11 represent the majority of cases in which fine-needle aspiration biopsy has been used.
The biopsy techniques of sclerochorioretinectomy of Peyman12,13 and partial lamellar sclerouvectomy of Shieldsl4 are the most common methods of combined local resection and excisional biopsy. There are many potential problems with extensive surgery, including vitreous hemorrhage, cataract, retinal detachment, suprachoroidal hemorrhage, and ocular hypotony. However, the combined biopsy and resection offers histologic confirmation and definitive management. The eye can often tolerate extensive surgery and maintain surprisingly good vision if vital structures are not involved. Eyes with lost visual potential, severe glaucoma, or pain should probably be removed.15 Newer methods of internal resection for malignant melanoma are currently under investigation and may eventually offer another treatment in our surgical armamentarium.2,16,17
IRIS
Many neoplasms may involve the iris, and clinical differentiation may be difficult. Most primary iris melanomas are benign in nature and often confused with leiomyoma and benign-appearing nevi.18 Patients harboring iris melanoma are younger than patients with melanoma of other parts of the uvea.19 The majority of iris melanomas fall into the category of spindle A–type melanoma and are slow growing, with only rare metastasis.20,21 In recent years, clinical observation of suspicious lesions for malignant features rather than immediate surgical resection has been advocated. Factors associated with metastasis in iris melanomas include increased age at diagnosis, increased intraocular pressure, posterior tumor margin location near iris angle or root, extraocular growth of the tumor, and prior surgical treatment.21 Fluorescein angiography has limited clinical value because both inflammatory and neoplastic lesions have prominent leaking vessels. Most authors agree that even when histologic examination of an iridectomy indicates a melanoma, complete excisional biopsy is adequate therapy. In view of this, fine-needle aspiration biopsy is usually reserved for either metastatic or inflammatory lesions when the diagnosis is in question.
GROWTH OF IRIS MASS
Tumor growth typically is slow and necessitates accurate serial photographic documentation. Pigmentary changes may occur for a number of reasons and should not be considered as evidence of definite growth. There is no evidence that there is a critical size of iris tumor prior to metastasis; however, any lesion greater than 2 clock hours usually involves the angle structures and require larger amounts of resection. Iris lesions closer to the iris root are more likely to involve the ciliary body and angle, necessitating an iridocyclectomy.
Heterochromia may indicate that the tumor more diffusely involves the iris stroma.22 Tumor seeds, spotted over the iris surface, also indicate a more diffuse nature. In certain instances, normal and abnormal iris areas cannot be clinically differentiated, necessitating multiple biopsy sites or a more radical surgical approach.22,23
IRIS LESIONS
In the last decade, iris biopsy has been used to diagnose iris lymphoma, leprosy, juvenile xanthogranuloma, leukemia, coccidioidomycosis, Lyme disease, and Refsum’s disease.24,25,26,27,28,29 Lack of tissue diagnosis does not preclude the presence of a neoplasm, even when performed at tertiary centers experienced in ophthalmic oncology.30
TECHNIQUE OF EXCISIONAL BIOPSY
The goal of surgery is to remove the malignant lesion en bloc without contamination and tumor seeding of the remaining tissue.21 The surgical approach is similar to extracapsular cataract extraction. Wide shelving of the incision should be avoided to allow adequate iris root exposure and complete excision. Sutures may be preplaced or placed later. A viscoelastic substance is used to protect the lens and the cornea from surgical trauma (Fig. 1A); however, adequate removal is necessary prior to wound closure. With the cornea retracted by the assistant, Barraquer or Vannas scissors are placed radially through the pupil and a cut is made up to the base on either side of the lesion in normal-appearing iris (Fig. 1B). The section of iris is grasped at the pupil margin, and fine scissors, usually curved Vannas scissors, are used to incise through the iris root (Fig. 1C). A similar approach for circumscribed iris lesions has been described by Shields and Shields,21,31 termed partial lamellar scleroiridectomy.
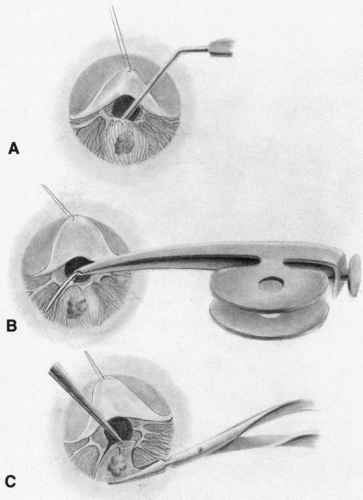 Fig. 1. A. Corneal-scleral wound is opened, and a viscoelastic substance is placed under the iris to protect the lens. B. The cornea is retracted by an assistant, and iris scissors are used to cut the tumor radially with clear margins. C. Iris section is grasped and excision along the iris root is performed. |
To achieve histologic orientation, the specimen should be pinned to a tongue depressor or piece of filter paper prior to placing into fixation solution. Fixed in this manner, proper anatomic margins of the tissue are preserved.
PROGNOSIS
The prognosis for vision is generally good in well-defined iris melanomas, providing surgical excision is without complications.23 Hyphema, corneal decompensation, cataract, and poor intraocular pressure control all can affect outcome. Cataract surgery may be combined with the excision of the iris lesions, but is usually postponed for secondary management. The prognosis for survival in iris melanoma excision is favorable with reported metastasis in less than 4% of patients,32 although more recent reports demonstrate 10% metastatic rates at 20 years.21 Rones and Zimmerman18 reported three deaths from metastases in 125 patients observed for as long as 15 years or more. Diffuse iris melanomas with heavy pigmentation are most likely to metastasize, particularly if nuclei show prominent nucleoli.
CILIARY BODY
Tumors and cysts may involve the ciliary body or be combined with iris lesions. These lesions include glioneuroma, medulloepithelioma, iridociliary cysts, leiomyoma, malignant melanoma, melanocytoma, lacrimal gland choristoma, adenoma of the nonpigmented ciliary epithelium, and nematode granuloma; it is sometimes difficult to differentiate them clinically.33,34,35,36 Congenital tumors are more often medulloepitheliomas or, rarely, glioneuromas, which present between ages 2 to 4 years with visual symptoms.37 In recent years, ultrasound biomicroscopy has proven to be a useful tool for diagnosis of iris, ciliary body, and anterior choroidal lesions.38,39,40,41,42 In cases that remain diagnostic dilemmas, iridocyclectomy is useful in permitting surgical excision of suspicious lesions without sacrificing the eye.33 Iridocyclectomy offers the benefit of both treatment and diagnosis as an excisional biopsy for lesions that are small and localized.
INDICATIONS FOR IRIDOCYCLECTOMY
Mass Lesion Growth
The option of observing a ciliary body lesion is determined by its initial status on presentation. Small lesions may be followed for growth if visual functions are intact; however, most melanomas43 and medulloepitheliomas44 result in early enucleation because of advanced stages at presentation with cataract, glaucoma, retinal detachment, and sometimes pain.
Small lesions confined to the iris and ciliary body may be successfully resected, usually when they produce symptoms or documented suspicious growth. Ciliary body melanoma often remains hidden and asymptomatic until attaining a large size, which may obstruct the visual axis or produce glaucoma.
Vail33 noted that iridocyclectomy may be performed with lesions not greater than 4 clock hours, although other authors have stated that lesions from 2.5 to 6 clock hours can be safely excised.20,33,45,46 Intraoperative and postoperative complications, particularly hypotony, are increased proportionally by the size of the tumor. Whether enucleation would result in better survival statistics than iridocyclectomy in larger melanomas is not known. Complications include seeding of the iris by iris melanoma and tumor recurrence.47,48 Thorough systemic and ocular examination should reveal no evidence of tumor extension or metastases prior to excision.
TECHNIQUE OF IRIDOCYCLECTOMY
Limbal Flap Approach
A fornix-based conjunctival flap is made to expose sclera in the area of the tumor. An anterior-hinged limbal-scleral flap is raised four-fifths of the scleral thickness at least 3 mm around the tumor (Fig. 2). Diathermy is applied to the remaining scleral bed surrounding the tumor. The anterior chamber is entered, and the flap is elevated to expose iris and tumor (Fig. 3). The tumor is excised starting at the pupil margin, moving posteriorly, and removing the section in one piece. The sector iridectomy is then closed with fine nonresorbable suture and the scleral flap is closed with interrupted sutures (Fig. 4).
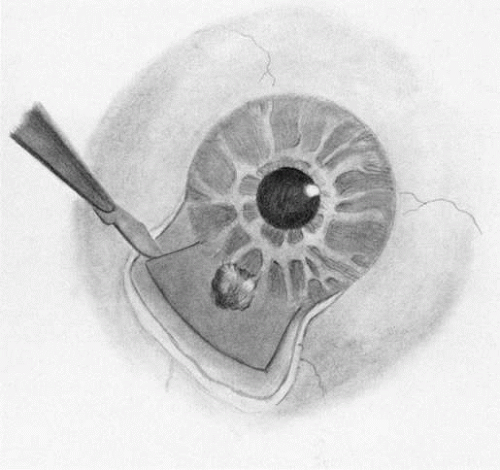 Fig. 2. Fornix-based conjunctival flap is opened. The scleral flap is raised four-fifths of the thickness 3 mm around the tumor. |
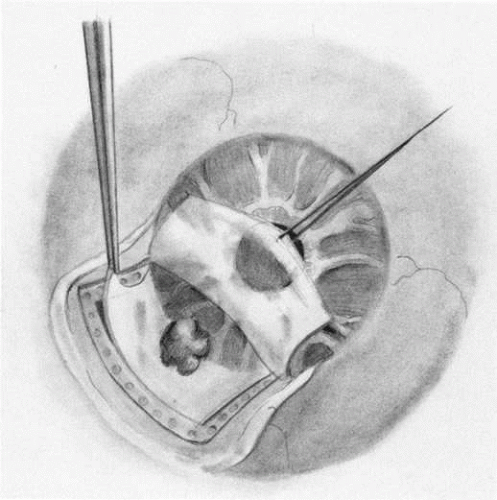 Fig. 3. Diathermy is placed in scleral bed. The tumor is excised. |
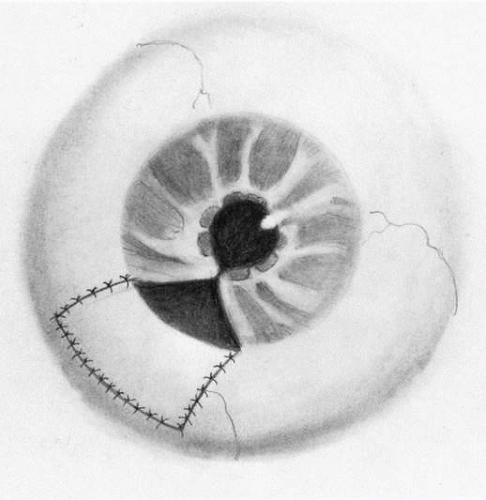 Fig. 4. Sector iridectomy and scleral flap are closed with fine interrupted sutures. |
T Incision of Stallard
The T incision of Stallard allows larger tumor exposure and excision. A conjunctival flap is opened to expose bare sclera and a Flieringa ring is fixed through episcleral sutures. A T-shaped limbal-scleral incision is then made with a knife and extended with the corneoscleral scissors. Closing sutures may be preplaced. The ciliary body surrounding the lesion is treated with penetrating diathermy (Fig. 5A). With the cornea and scleral flaps reflected, the pupillary margin is grasped and the iris incised radially to the iris root (Fig. 5B). The involved portion is excised with scissors.49,50
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


