Fig. 1
Task trainer model of upper airway. This photo shows the view of the manikin’s vocal cords as seen during intubation.
There are many options for simulation manikins available on the market that range in cost from a few hundred to several thousand dollars. The fidelity, or technological capability, of a manikin refers to how closely the model represents an actual patient. A high-fidelity patient simulator incorporates a manikin upon whom procedures such as intubation and chest tube placement can be performed, as well as physical exam findings that can be manipulated, and real time vital sign monitors that are controlled by computer software. The available software programs allow the simulation facilitator to change the manikin’s physical exam findings and vital signs as the clinical scenario progresses. Centers with high-fidelity simulators often perform simulations in situ or have a space set up to resemble their unit’s standard patient room or resuscitation room to add realism (Fig. 2).

Fig. 2
High fidelity simulation center. This simulation center has a high-fidelity manikin connected to monitors and controlled by a laptop. The standard neonatal bed space includes a warmer bed, ventilator, IV poles and a bedside cart. In the upper left is a camera for recording simulation for later review
Low-fidelity simulators span a wider range of options but do not have integrated software or electronics. In its most basic form, a low-fidelity simulator may be a simple doll or homemade approximation of an airway. Low-fidelity options on the market range from manikin head task trainers to full body manikins with many interactive features for the learner such as inflatable lungs to simulate ventilation. Both the homemade and purchased manikins can be modified to create difficult airway models (Table 1). Both low- and high-fidelity manikins can also be used to practice intubation in nonstandard positions, such as might be needed for a patient with an open neural tube defect or after spinal surgery [16] or with conjoined twins (Figs. 3 and 4).


Table 1
Manikin modifications of difficult airways
Condition | Goal | Modification |
|---|---|---|
Subglottic stenosis | Narrow airway below vocal cords | Apply external pressure to trachea with zip-tie or insert putty below vocal cords |
Laryngospasma | Narrow airway above vocal cords | Apply external pressure to airway above vocal cords |
Macroglossiaa | Provide an obstruction in the oral cavity | Overfill the manikin tongue or add volume to the outside of the tongue |
Meconium in the airway or airway bleeding | Obstruct the view of the vocal cords with an opaque substance | Insert thinned paste dyed green or red into the oropharynx |
Micrognathia or Pierre Robina | Increase difficulty with jaw retraction and view of the vocal cords | Move manikin jaw posterior to standard position |
Enlarged epiglottis | Obstruct the view of the vocal cords with the epiglottis | Apply putty to enlarge or elongate epiglottis |
Unable to bag mask ventilate or intubatea | Force learner to perform cricothyroidotomy | Replace airway below vocal cords with disposable tubing/skin covering and/or use putty to fully obstruct airway |
Cervical tumor/massa | Obstruct the view of the vocal cords, restrict neck movement | Insert bean bag or firm mass under skin of manikin’s neck, pushing on airway |
Cervical spine immobilitya | Restrict available movement of airway | Place cervical spine brace around manikin’s neck |
Spinal condition requiring side-lying position | Intubation in nonstandard position | Turn manikin on side |
Tracheostomy tube obstructiona | Force learner to remove/replace tracheostomy tube | Occlude tracheostomy tube lumen |
Fig. 3
Side-lying intubation. This manikin has been modified to have an open neural tube defect, forcing the learner to intubate in a nonstandard position
Fig. 4
Conjoined twin intubation. In this scenario two manikins were used to simulate the anticipated delivery of omphalopagus conjoined twins, allowing the team to practice airway management prior to delivery
One high-technology option for simulation is virtual patients. Software can be used to model the human airway and adjust the view on screen depending on input from the user. The model can be created from 3D reconstructions of actual patient airways or built from scratch to demonstrate a particular condition. The user input can be obtained from a laryngoscope wired to sense the user’s movements so that the screen view changes based on the accuracy of their movements. A virtual model constructed from 3D CT scan images has been shown to be as effective as a manikin for intubation training [17]. This technology permits educators to make airway models from CT scan images of real patients with difficult airways or airway malformations, allowing multiple trainees to get experience from one patient without risk to the actual patient.
Cadaver and animal airway models have high rates of satisfaction among learners, as they have been shown in small studies to improve patient level outcomes [10]. There are no reported studies of neonatal cadaveric models for intubation, but in adult models, fresh frozen cadavers have the highest rate of realism for intubation [18]. Animal model programs have reported using ferrets and piglets to simulate the neonatal airway. This technique is generally considered safe for the animals and adds a significant level of realism to the encounter without any risk to human patients. This method can be used to train clinicians in the intubation of patients with normal airways but is less useful in difficult airway management. Technology-based strategies can help to improve the learning experience using many different types of airway trainers.
Bag Mask and Alternative Airway Training
Infants with difficult and critical airway issues may not be able to be intubated at delivery or presentation to care, even by experienced airway personnel. For these fragile infants, provider proficiency with bag mask ventilation (BMV) and alternate airways can mean the difference between survival and death. During a 6-month period of neonatal training, one group of Australian residents had an average of 17 opportunities to provide BMV [17]. In the current American pediatric training model most residents will get only 2–3 months of training in neonatal care, potentially reducing their opportunities to learn and practice this life saving skill to less than ten instances throughout residency. Opportunities for use of alternative airways, such as a laryngeal mask airway (LMA), are even less frequent. As with other airway procedures and tools described in previous sections, lack of familiarity and infrequent use can result in poor performance of a task. In a study of the effectiveness of resident positive pressure ventilation (PPV) delivery to preterm infants, one quarter of the resuscitations demonstrated significant airway obstruction during PPV, and another quarter were noted to have significant mask leaks [18]. Simulation manikins can provide an important opportunity to practice these life saving skills. For experienced providers, manikin demonstration is more effective at decreasing mask leak during PPV then watching simple instructional videos [21].
BMV is a critical component of the NRP algorithm and the first step in resuscitating a depressed infant. Both low- and high-fidelity manikins can be used to practice BMV and LMA placement. Providing adequate BMV requires correct hand placement, correct mask position on the neonate’s face, adequate jaw thrust, and appropriate pressure on the mask (Fig. 5). All of these tasks can be assessed on a manikin. High-fidelity manikins may also be able to record the volume or pressure of the delivered breaths to provide feedback regarding the effectiveness of the mask seal and delivered inspiratory pressures [22]. Providers must be able to troubleshoot mask air leaks and airway obstruction during BMV. Even in the hands of experienced providers, neonatal facemasks can still have significant air leaks that compromise ventilation [23]. The steps to resolve inadequate ventilation described in NRP follow the acronym “MR SOPA” and include: mask and patient repositioning, suctioning, opening the mouth, increasing pressure, and considering an alternative airway support device [3]. Manikins with articulating jaws and realistic upper airways can provide an important opportunity to practice these steps, including the use of alternative airways.
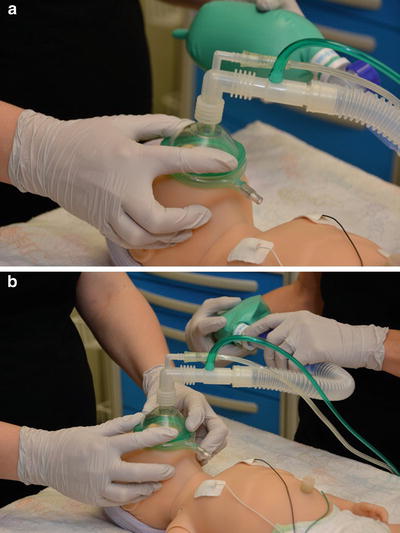
Fig. 5
Bag mask ventilation techniques. (a) One person BVM demonstrating correct hand and mask placement. (b) Two person BMV demonstrating correct hand and mask placement
The LMA has been shown to be effective for establishing ventilation and resolving bradycardia in the delivery room [24]. LMAs are simple to insert and come in many sizes. A size 1 LMA is approved for use in infants less than 5 kg and there are reports of its successful use in premature infants as small as 1.1 kg [25]. As residents may be the only providers present at a delivery and have low reported success with endotracheal intubation, an LMA may provide a safe temporizing measure while advanced airway providers are called to the bedside. LMAs also have a major role in stabilizing infants with difficult or critical airway conditions, such as cervical neck masses (Fig. 6).
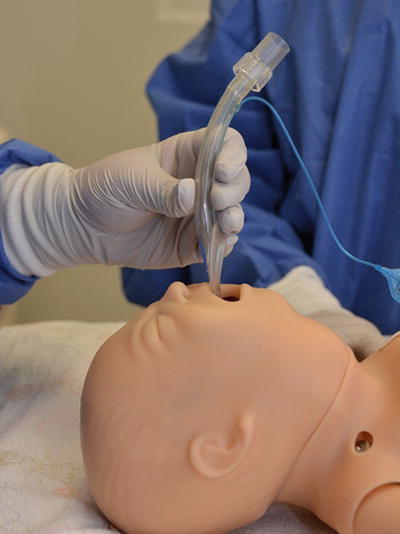
Fig. 6
LMA insertion. This manikin has been modified to have a difficult airway due to cervical neck mass requiring the learner to use an LMA
Nasopharyngeal and oropharyngeal airway insertion should also be included in airway training programs. Nasopharyngeal (NP) airways use a tube inserted in one nostril that opens a conduit between the nostril and the nasopharynx above the level of the epiglottis and can be used to bypass obstructions at the levels of the nose, nasopharynx, and base of the tongue. Oropharyngeal (OP) airways use a small piece of curved plastic inserted into the unconscious patient’s mouth that bypasses obstructions at the base of the tongue. Both NP and OP airways can be inserted into term or near-term neonates and can be combined with BMV to achieve adequate ventilation when intubation is not possible. These devices are especially useful in infants with micrognathia, such as in Pierre Robin Syndrome, who may present unexpectedly at delivery. As both of these devices can be inserted quickly and easily, it is imperative that trainees be proficient in their use in case of an emergency. Most airway manikins can be used to practice NP and OP airway insertion, and all delivery room providers should practice their insertion regularly to maintain competence.
Intubation Training
Learning and maintaining proficiency for complex procedures like endotracheal intubation can be divided into two steps: a cognitive step and a psychomotor step [26]. The cognitive step is a period devoted to learning about the procedure and developing an understanding of the indications, contraindications, and motor actions involved. Cognitive steps about intubation should include a review of normal and abnormal anatomy, types of equipment needed, and the procedural steps. The important strategies of didactic learning include cognitive engagement, repetitions, feedback and variety [27]. Learners can be cognitively engaged by interactive teaching, such as walking through case examples, asking questions, and using videos or live demonstrations. Although didactic teaching alone is often insufficient for procedural training, a well-designed and executed class can add important layers to a provider’s understanding of a process. For instance, knowing the names of anatomic landmarks aids communication during a difficult procedure, and understanding airway mechanics can aid in provider decision-making during emergencies. For these reasons, didactics should be integrated into simulation-based learning to maximize understanding.
The psychomotor step of procedural training involves practicing the procedure with correction and reinforcement. Allowing the trainee the opportunity for practice of the procedure in a safe learning environment using a partial task trainer, manikin, or virtual-reality training is known to be superior to traditional clinical medical education in achieving specific skill acquisition (Fig. 7) [27]. Instructional design features shown to improve simulation-based training can easily be incorporated into simulation training for endotracheal intubation. These include group practice, individualized learning, mastery level training, and variation in task complexity [27]. Repetition and instructor feedback remain crucial learning strategies, regardless of the training methodology.
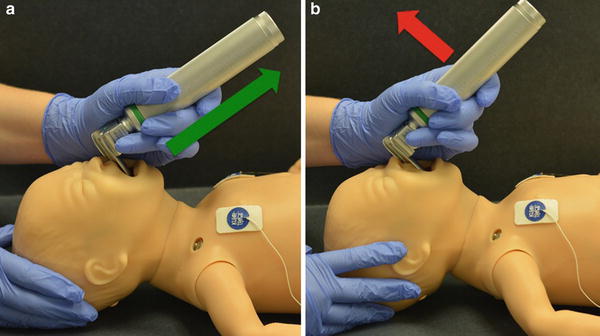
Fig. 7
Using a manikin to practice intubation. This airway manikin is being used to practice the physical skills of intubation. (a) Correct laryngoscope positioning, proper arm movement shown with green arrow. (b) Incorrect laryngoscope positioning restricting view of the airway, improper arm movement showing rocking of the laryngoscope shown with red arrow
Teamwork skills for intubation can occur in a multidisciplinary setting. During a standard intubation in the ICU there is a provider skilled in airway management, a bedside nurse, and a respiratory therapist. All of these people have individual roles that must integrate tightly together to successfully manage an airway emergency. A multidisciplinary intubation simulation could include a nurse who administers rapid sequence intubation medications and monitors vital signs, a respiratory therapist who prepares the equipment and secures the endotracheal tube, and a front line clinician who organizes the group and performs the procedure. By practicing these skills together, the team of care providers can improve communication, efficiency, and patient safety. Group practice can also be used to train a group of front line clinicians where each provider takes a turn in the different roles. This gives each person a chance to practice skills outside of his or her usual scope, which may be important as it provides perspective on communication and teamwork.
Individualized learning can take place both within the group practice model and in one-on-one instruction. Using this method, an individual learner’s specific needs or deficiencies are identified, and the learner uses deliberate practice with facilitator input to improve his or her performance (Fig. 8). As defined by Ericsson, deliberate practice describes a regimen of effortful activity designed to optimize improvements in the acquisition of expert performance [29]. Deliberate practice with intubation simulations has been shown to improve resident success with intubation [29]. Deliberate practice can also be used to remediate individuals or provide additional experiences for learners that require additional training. For instance, if fellows in Neonatology programs identify the desire to have more practice with intubations, they can have individualized learning programs to practice intubation with different manikins and task trainers in both conventional and unconventional settings.

Fig. 8
Deliberate practice with facilitator. The facilitator provides instruction to help the trainee learn to intubate the manikin
One critical component to intubation training is variation in procedural complexity. Once trainees have demonstrated proficiency at standard intubation, they should be challenged with increasingly complex scenarios to solidify their skills. Even intubation of the normal infant airway can be made more complex by varying the scenario to include different disease processes, different clinical environments, and a range of equipment availability. Specific intubation skills such as endotracheal tube replacement and nasal intubation should be rotated through the varied scenarios.
Endotracheal tube replacement can be used for upsizing the tube diameter or to remove a plugged tube. Patients requiring tube replacement may be too unstable to tolerate prolonged time without an artificial airway and so may not tolerate the time required for an existing endotracheal tube to be replaced. The procedure requires practice, because the timing element and coordination of steps can be difficult to manage. For example, in an endotracheal tube replacement scenario, the patient may be ventilating poorly due to a large air leak around a small endotracheal tube. The team would need to recognize that patient decompensation was due to improper tube size, choose an appropriate sized replacement tube, coordinate a secondary person to stabilize the existing tube, obtain an adequate view of the vocal cords, and coordinate the tube exchange while minimizing the length of time without ventilation. Multidisciplinary practice of this type of scenario is important, as it often requires a nurse or respiratory therapist to assist with the endotracheal tube replacement.
Another advanced airway skill amenable to simulation training is nasal intubation. Nasal intubation is ideal for patients with excessive oral secretions, surgical wounds in the mouth, older infants requiring prolonged intubation, and patients with facial malformations precluding proper oral tube securement. Some intensive care units may even use this as their primary method of endotracheal intubation. As such, all airway providers should be trained to perform nasal intubation. This procedure varies from traditional oral intubation in equipment and sequence of events. Magill forceps are unique to nasal intubation and unfamiliar to many providers. After inserting the endotracheal tube through a nare and advancing the tube down into the larynx, the provider uses a traditional laryngoscope to view the vocal cords while actively placing the endotracheal tube into the airway using Magill forceps (Fig. 9). Newer techniques using ENT “cupped ear” forceps allow easier instrumentation of the oral airway to facilitate nasal intubation in smaller infants. These forceps are jointed at the end of the device, limiting trauma to the epiglottis and other airway structures (Fig. 10). Many airway task trainers and high-fidelity manikins have patent and anatomically correct nasal passages for use with nasal intubation, providing a valuable training experience for a rare intubation event.
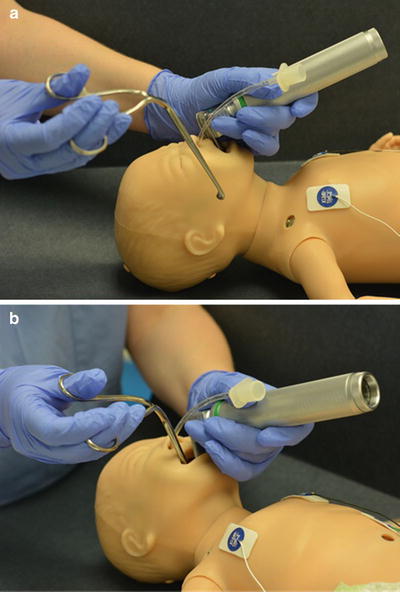
Fig. 9
Nasal intubation. (a) The provider prepares the manikin for nasal intubation by placing the endotracheal tube in the nare and obtaining a view of vocal cords using direct laryngoscopy. (b) The provider inserts the Magill forceps into the mouth, using them to guide the endotracheal tube through the vocal cords

Fig. 10
Cupped ear forceps are more useful for nasal intubation for smaller neonates and infants than the larger MaGill-type forceps. Significantly small and longer with the movable joint at the tip allows for easy grab of the ETT
Training programs often need to show that their graduates have adequate experience to practice independently and thus have designed procedure log systems to track both the frequency and success of trainee procedural attempts. As intubation experiences become increasingly rare, programs may need to find alternate ways to show regulatory agencies that they are producing clinicians who have mastered advanced airway management. One way to assess proficiency with procedures is through simulation-based mastery learning (SBML). SBML sets a predetermined minimal passing standard (e.g., “mastery level”) and has several key characteristics which include practice that is focused on reaching mastery level performance, skill testing to assess achievement of mastery level performance, and continued practice, as needed, until the mastery level performance is achieved [31]. SBML can be used to verify proficiency with both commonly and uncommonly performed clinical and procedural skills. SBML augments deliberate practice through the addition of a clearly delineated level of performance that defines “mastery” with a given procedural skill and the requirement for continuous practice until mastery level performance is achieved [32]. Additionally, scenarios promoting mastery level skills should strive for realism; for intubation training this should include a realistic airway model, standard unit airway equipment, and airway personnel. Success metrics should include a time element and measures of communication, teamwork, and technical proficiency. A well-designed simulation program can be used to verify mastery level skills and can serve as evidence of proficiency for regulatory agencies.
Video Enhanced Laryngoscopy
The field of intubation has had many technologic advances. Using traditional direct laryngoscopy, only the user is able to see the airway; there may be delayed or no feedback regarding the success of the procedure, and there is no way to review the procedure after the event. New models of video or fiberoptically enhanced laryngoscopes allow more than one provider to see the airway. If the device has recording ability, it allows trainees to review their performance at a later time with supervisor feedback. In these devices a camera or fiberoptic scope sits near the light source on the laryngoscope blade and shows a magnified view on either a screen attached to the handle or a separate monitor. This method of intubation also improves awareness of procedural success since trainees have an enlarged view of the airway as the endotracheal tube is introduced. Furthermore, providers can receive feedback in real time about their skills. Even in experienced airway providers, fiberoptic and video laryngoscopes improve airway view grades [33] (See chapters “Anesthesia Challenges for the Difficult and Critical Neonatal Airway and Airway Emergencies in the Neonate: Preparedness at the Bedside” for full video laryngoscopy details).
Video and fiberoptic intubation devices can also be combined with patient manikins, both for task training and for use in larger airway emergency scenarios. This method of teaching advanced airway skills has been shown to be beneficial in the adult field. Anesthesia and Internal Medicine residents trained using a simulation manikin showed significantly better success in live patient intubation and time to intubation with a fiberoptic laryngoscope compared to residents trained via lecture from expert airway providers [34].
Identifying abnormal anatomy is an important step in the training of advanced airway providers such as anesthesiologists and intensivists but patients with these conditions are infrequently seen in standard practice. For rare airway anomalies, a video taken from within the airway, such as with a fiberoptic laryngoscope or flexible bronchoscope, allows multiple trainees and providers to learn how to recognize and manage the airway condition. Dynamic video recording can aid in the diagnosis of functional airway issues such as vocal cord paralysis or airway malacia [34]. This method is often employed in Otolaryngology training programs, where video recording of procedures is common but is rarely utilized by nonsurgical providers.
Tracheostomy Training
Infants with tracheostomies represent a very small proportion of the population but are frequently encountered in the intensive care units and operating rooms. They are a particularly vulnerable group of patients, as many have critical airway issues or severe lung disease. The National Audit Project of the Royal College of Anesthetists and the Difficult Airway Society emphasized the importance of tracheostomy care by stating: “displaced tracheostomy, and to a lesser extent displaced tracheal tubes, were the greatest cause of major morbidity and mortality in [the] ICU” [36]. To mitigate this risk, medical providers need to be familiar with the care and management of patients with tracheostomies, yet one-third of pediatric, non-otolaryngology healthcare providers rate their comfort with tracheostomy care as poor. Knowledge of tracheostomy tube management, even for advanced providers such as anesthesiologists, remains inadequate. In a series of questions regarding the care of tracheostomies, anesthesia residents scored only slightly higher than 50 % correct [37]. Fortunately, even one experience with changing a tracheostomy tube as a resident is correlated with a significant increase in comfort with the procedure [38]. Simulation provides a means to address these knowledge and skill deficiencies [39].
Many manikins can be modified or purchased to simulate an infant with a tracheostomy. Tracheostomy manikins can be used to practice technical skills such as tracheostomy tube changes or used in more elaborate simulation scenarios. Tracheostomy scenarios can include obstruction, dislodgement, or retrograde intubation depending on the discipline and level of the learner. Beginners may benefit from learning to provide PPV via a tracheostomy tube and performing a simple tracheostomy tube replacement. More advanced providers may benefit from practicing the management of a scenario in which a newly placed tracheostomy tube is dislodged and cannot be replaced.
Providers of all levels, from nurses to intensivists, should be familiar with simple tracheostomy tube care, making this an ideal topic for multidisciplinary simulation training. For example, a multidisciplinary scenario might start with a tracheostomy tube obstruction which progresses to bradycardia despite nursing efforts to suction and provide PPV via the tracheostomy. This scenario could require the resident or front line care provider to attempt a tracheostomy tube change and evolve to a full team code after the tracheostomy tube cannot be replaced through the stoma. Scenarios such as this happen infrequently in most institutions but carry a high risk of morbidity and mortality, especially in inexperienced hands.
Specially trained teams and protocols for how to manage emergency tracheostomy situations are starting to be used in institutions with high volumes of tracheostomy patients. Simple protocols regarding suctioning depth and pressure can improve patient safety [40]. Additionally, staff specially trained in tracheostomy care, such as nurse specialists or dedicated multidisciplinary teams can greatly improve outcomes in patients with tracheostomies with regards to complications and ICU admissions [40, 41]. Many of these care protocols and multidisciplinary teams are lead by Otolaryngology specialists who have the most experience in managing patients with critical airways. Once a protocol or team is created, disseminating the information can be accomplished through simulations with bedside nurses and front line care providers. As the care protocols and team assembly may rarely be needed, ongoing simulation provides a means to maintain a safe level of knowledge and skills.
Difficult Airway Management Simulation
Simulation allows for directed learning in an environment that is both safe for the learner and poses no threat to patient safety. Even a low-fidelity manikin can add realism to an airway emergency scenario. Appropriately designed simulations using high-fidelity simulators can come very close to the high pressures of a life-threatening emergency. In a large meta-analysis, simulation was found to be the superior method for teaching advanced airway management skills such as direct and fiberoptic intubation and surgical airways [10]. Manikins improve learner comfort with routine airway management and interventions, which can be translated to management of the difficult or malformed airway. For example, BMV, an essential skill for NRP algorithms, can be more challenging to perform effectively in an infant with severe micrognathia.
Each simulation scenario can be geared towards specific learning goals. A scenario may focus on procedures such as BMV, management of specific conditions such as subglottic stenosis, or on nontechnical skills of an airway code like teamwork and communication. Each type of scenario can also be tailored to different learner levels and disciplines (Table 2). During a scenario, if a learner is struggling with an objective, the facilitator can pause the scenario, provide immediate feedback, and then restart the simulation to allow the learner to improve upon his or her performance. Important advantages to simulation training include the ability to recreate a difficult or rare clinical presentation, allowing the trainee or team to redo the event with feedback, and for trainees to experience and practice the management of a rare event, especially if it has not been previously encountered during training.
Table 2
Airway simulations for different levels of training
Trainee level | Example scenario | Goals | Objectives |
|---|---|---|---|
Medical student | • Baby with small jaw presenting for a preoperative visit prior to hernia repair | • Identify risk | • Recognize significance of exam finding |
• Anticipate issues | • Identify risk of airway obstruction | ||
• Teamwork | • Anesthesia or ENT consult prior to OR | ||
Nurse or respiratory therapist | • Infant with worsening stridor | • Recognize signs of respiratory distress | • Recognize stridor |
• Use airway stabilizing maneuvers | • Attempt airway repositioning | ||
• Call for help at appropriate time | • Use bag mask appropriately | ||
• Use code bell to get help | |||
Resident/front line clinician | • Delivery of infant with prenatally diagnosed Down syndrome | • Prepare for delivery | • Anticipate risk of airway issue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|