• Concentration 1:10,000 (0.1 mg/mL)
• ETT dose is 0.5–1 mL/kg
• UVC/IV dose is 0.1–0.3 mL/kg
• Follow with a 0.5–1 mL flush NS
• Re-check heart rate after 1 min of compressions and ventilations
• Repeat dose every 3–5 min
It is important to note that while actual anatomical details such as cervical neck masses give a direct clue towards the likely airway obstruction, other findings maybe more indirect and thus evade an easy association. These indirect clues may arise as a consequence of airway obstruction, such as hydrops or polyhydramnios. They may also be part of a syndrome of which airway obstruction is a feature. A good example of this is coexistence of structural heart anomalies and coloboma in a fetus may alert the provider to the possibility of choanal atresia as part of the CHARGE syndrome (previously thought to be an association). As such existence of major congenital anomalies should raise the index of suspicion for airway anomalies as part of a global pathology. Other syndromes such as Treacher Collins, Goldenhars and Pierre Robin syndromes can also present with significant airway obstruction due to the severe micrognathia. Common diagnoses associated with neonatal airway obstruction that may present in the delivery room are listed in Tables 2, 3 and 4.
Table 2
Special considerations for preterm neonates
1. Increase temperature of the delivery room to approx. 25–26°C (77–79°F) |
2. Polyethylene plastic wrap |
3. Place portable warming pad under the layers of |
4. Towels at the radiant heat warmer |
5. Use blended O2 |
6. Consider CPAP for good heart rate but an increased work of breathing |
7. May need to administer surfactant for preterm infants intubated for respiratory distress syndrome or RDS |
Table 3
Prenatal ultrasound finding associated with neonatal airway obstruction. Congenital high airway obstruction, (CHAOS)
Non-immune Hydrops—severe neck edema |
Polyhydramnios with tracheal atresia |
Severe Micrognathia-craniofacial/genetic syndromes |
Large echogenic fetal lungs-upper airway obstruction |
Dilated airways with stenosis |
Cervical lymphangiomas/teratomas |
Neuromuscular condition with arthrogryposis and jaw immobility |
Table 4
Common causes of neonatal airway that may present in the delivery room setting
Conditions associated with extrinsic compression of the airway |
1. Cervical lymphatic malformation (cystic hygroma) |
2. Cervical teratoma |
3. Associated with mandibular hypoplasia: |
(a) Pierre Robin sequence (Stickler syndrome) |
(b) Nager Syndrome |
(c) Treacher Collins Syndrome |
(d) Bilateral hemifacial microsomia—Goldenhars Syndrome |
4. Associated with macroglossia |
(a) Down’s Syndrome |
(b) Beckwith Weidmann Syndrome |
(c) Lymphangioma |
Conditions associated with intrinsic airway compression |
1. Lingual thyroid |
2. Vallecular cyst |
3. Others, such as Nasal encephalocele, ranula, glioma, dermoids, etc. |
Intrinsic airway obstruction |
1. Choanal atresia/stenosis |
2. Tracheal agenesis/stenosis |
3. Laryngeal agenesis/stenosis |
4. Congenital high airway obstruction sequence (CHAOS) |
5. Vocal cord palsy (primary condition, associated with hydrocephalus) |
6. Laryngeal web |
7. Tracheomalacia/Laryngomalacia |
However, during intubation, conditions affecting the supra, glottic and subglottic area may only then become obvious and hinder the neonatologist from routine intubation. Conditions such as subglottic stenosis, masses, vocal cord paralysis, or atresia can be uncovered in the delivery room.
Airway Emergencies in the Delivery Room
Specific airway-related diagnoses, such as listed above likely mandate a customized approach to neonatal resuscitation. Another group of conditions that deserves a special mention here, comprise conditions that are not directly associated with a specific airway diagnoses, nevertheless have implications for airway management in the delivery room. These mainly include conditions wherein the role of bag-mask ventilation is limited and prompt orotracheal intubation is recommended for example, esophageal atresia, and congenital diaphragmatic hernia.
Once an airway obstruction has been identified, the fetus needs to be evaluated for other possible coexisting conditions. The airway obstructions maybe an isolated finding or part of a global/syndromic condition. The latter raises serious ethical questions as more neonates with severe birth defects are now being born at Children’s Hospitals with immediate access to subspecialty services Figs. 1, 2, 3 and 4.
show how organization and practice can prepare for an airway emergency.
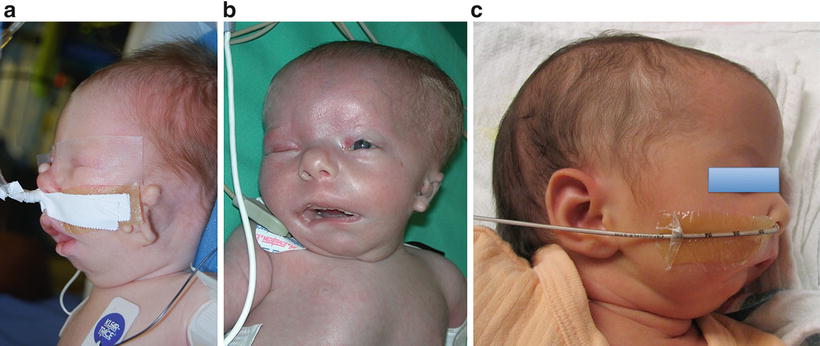
Fig. 1
(a–c) Goldenhars Syndrome with severe micrognathia and airway obstruction requiring specialized airway management in immediate birth period
Fig. 2
Delivery room airway emergency algorithm:**Courtesy of Michael Posencheg, MD, medical director of the Hospital of the University of Pennsylvania neonatal unit. **
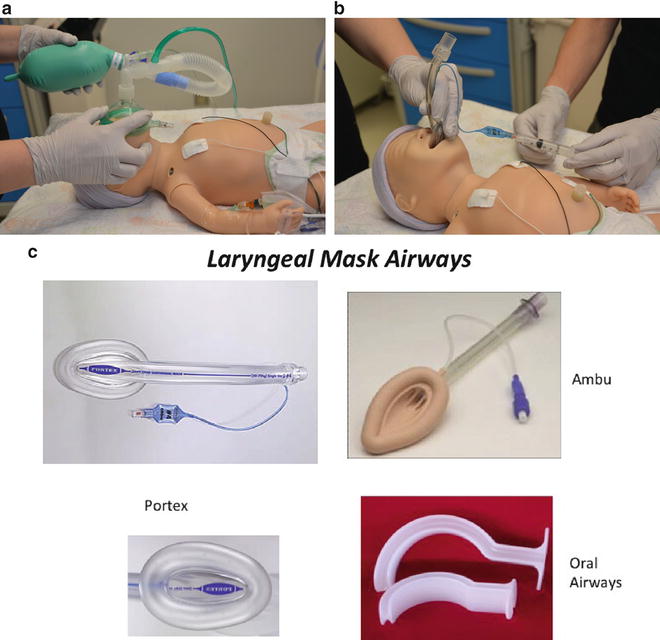
Fig. 3
(a) BMV placement in a neonate. (b) LMA Placement in a neonate. (c) Different LMA types
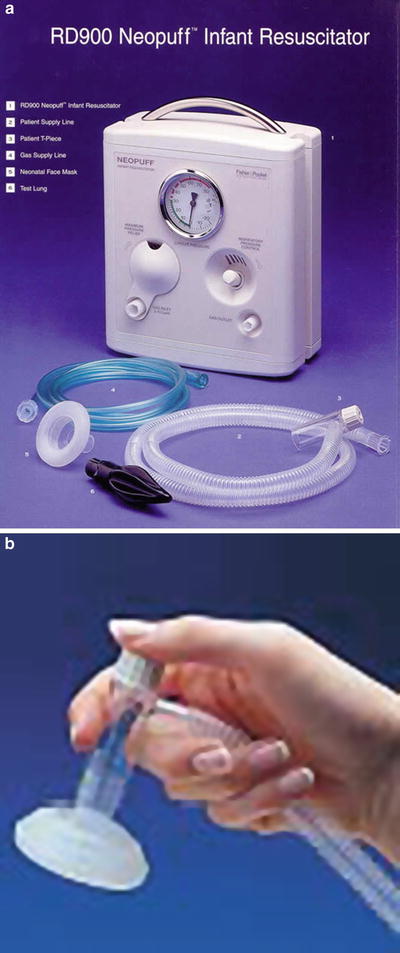
Fig. 4
(a) The Fisher Paykel NEOPUFF RD 900 Neopuff™ Infant Resuscitator. (b) Use of the mouthpiece with the Neopuff™ Infant Resuscitator
Timing and Mode of Delivery
Understandably, the identification of fetal airway obstruction has significant implications for the plans surrounding the delivery. As with many other complex congenital anomalies, cases with suspected fetal airway obstruction should be referred for further evaluation to a tertiary center. Ideally such a referral center should have dedicated, multidisciplinary teams with advanced neonatal, otorhinolaryngology and pediatric surgery services with experience in fetal/neonatal airway issues. The course based on the diagnoses may comprise minimal noninvasive support to requiring EXIT delivery [5]. (Discussed in Chapters “Prenatal Assessment and Perinatal Management of Suspected Airway Compromise in the Fetus and Neonate” and “Operative Surgical Management of Fetuses with CHAOS, (Congenital High Airway Obstruction Syndrome): Management at Delivery”). The timing and choice of delivery will also be influenced by fetal and maternal health, particularly in cases of fetal hydrops and/or maternal “mirror syndrome” [6]. The most important thing when there is time to prepare is having experienced pediatric ENT present with full service tracheostomy tray and set up. Everyone should be prepared Figs. 5, 6, 7, 8 and 9.
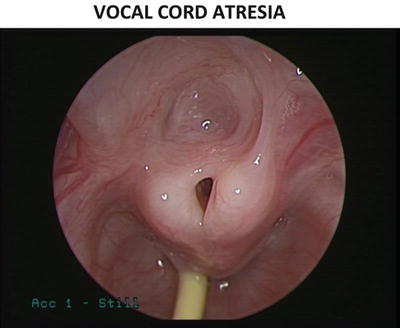
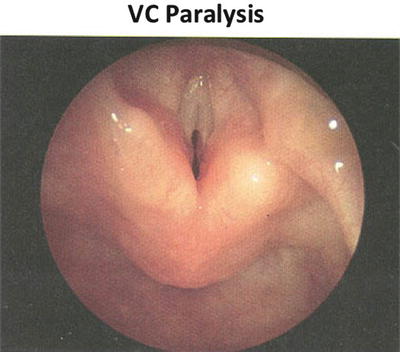
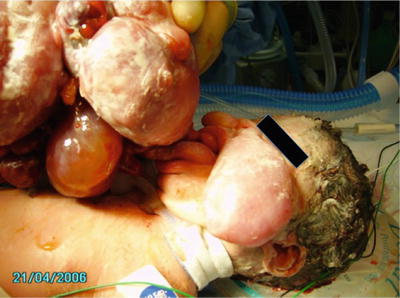

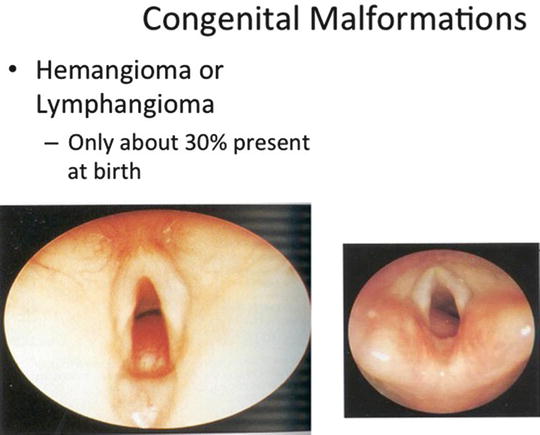
Fig. 5
Vocal Cord atresia causing airway obstruction during intubation
Fig. 6
Vocal Cord paralysis causing airway obstruction at delivery
Fig. 7
Epulis/Epignathus causing acute oral obstruction and an airway emergency at birth Tracheostomy may be the only treatment for these types of obstructions
Fig. 8
Giant lymphangiomas causing acute oral obstruction and an airway emergency at birth Tracheostomy may be the only treatment for these types of obstructions
Fig. 9
Laryngeal Hemangioma or Lymphangioma can easily obstruct the entrance to the glottis and only be found upon intubation in a neonate with respiratory distress
Postnatal Diagnoses
In situations where the diagnoses of airway obstruction are not available or suggested prenatally, the clinician can get valuable information from the delivery room experience.
Respiratory distress, especially when unresponsive to routine resuscitative measures, is always an obvious presenting complaint of significant airway obstruction. Externally visible masses and dysmorphic features suggestive of micrognathia and/or retrognathia [7] can be important clues. Other such symptoms may include excessive secretions, stridor, and inability to pass suction catheters through one or both nostrils Figs. 10, 11, 12, 13 and 14.


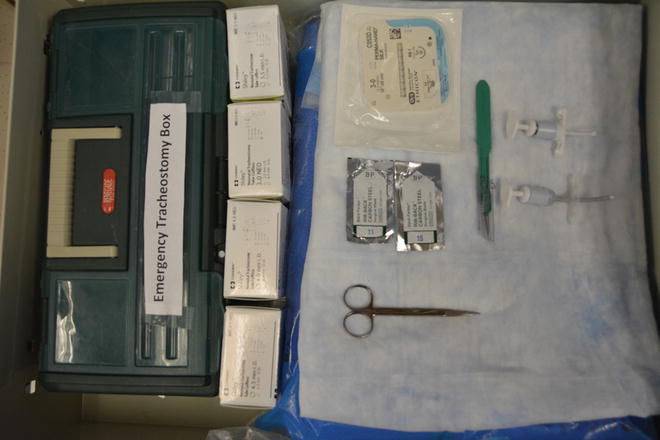


Fig. 10
Standard type neonatal delivery room critical airway cart
Fig. 11
Emergency set up of delivery room resuscitation
Fig. 12
Emergency tracheostomy set up
Fig. 13
Essential basic delivery room airway equipment: LED laryngoscope handles and blades, LMAs, ETTs, masks, ETTs, and stylettes
Fig. 14
Videolaryngoscopy: Glidescope and Storz CMAC now available for neonatal patients with size 0 and 1 blades
Birth Trauma
Finally, the possibility of birth trauma causing airway obstruction or impairment should be considered. This is especially true for macrosomic neonates with history of prolonged shoulder dystocia. While, such delivery circumstances may result in perinatal asphyxia, the clinician should still be cognizant of the possibility of airway trauma. Cases of tracheal or laryngeal tears are rare but have been reported in the literature [8, 9].
Summary of Delivery Room Management
Benefits exist in standardizing the care patients receive. We have discussed how things should be done in the delivery room regarding thermoregulation, oxygen titration, and respiratory support. However, the infrastructure to perform these interventions including who should perform which tasks requires some more detail. Understanding that we are trying to provide the best medical care, while training residents and fellows. We recommend the following guidelines to establish roles and responsibilities:
1.
Establish a team leader—this person is usually a fellow for attending.
2.
Airway—experienced personnel, usually a senior front line clinician, fellow for attending.
3.
Umbilical Lines—should have an experienced person assisting residents to balance efficiency with training.
4.
Nursing—at least one for baby (thermoregulation) and one recording. If possible, an additional medication nurse is optimal.
5.
Respiratory Therapy—Need a dedicated person to manage CPAP nasal interface and oxygen titration. Surfactant administration if applicable.
6.
Limit traffic—personnel without roles should leave the room, with rare exception. Attempt to keep doors closed to maintain room temperature.
7.
Be prepared to handle unexpected situations arising out of unanticipated airway emergencies. Simple cues on physical exam and history maybe very important to direct management.
8.
In cases of unexpected airway emergencies, understand your resources and involve specialists in a time-sensitive manner. Other teamwork guidelines apply with more focused communication and heightened sense of urgency.
Section 2: Resuscitation in the Emergency Department
Nathan W. Mick and Joshua Nagler
Background
Neonatal airway management in the Emergency Department (ED) is an infrequent but critically important skill for emergency medicine providers. The psychomotor skills required to perform laryngoscopy and intubation in a neonate are similar to those utilized in the care of an older child or adult. However, there are key anatomic and physiologic differences between these disparately aged patient populations, which are most pronounced in neonates who are at the youngest end of the pediatric age spectrum. These differences impact the indications for airway management and necessitate modifications in approach.
Emergency medicine providers are further challenged by a relative inexperience in caring for critically ill neonates. Those with fellowship training in pediatric emergency medicine may have some additional experience from their neonatal and pediatric intensive care rotations as well as scheduled training in the operating room setting. However, the vast majority of neonatal intubations in EDs occur outside of a tertiary care children’s hospital by providers with limited and often remote pediatric training. Nonetheless, neonatal and pediatric “readiness” is an essential component of general ED operations. Fortunately, most emergency medicine providers will have comfort in recognizing critical illness and responding quickly; however, there are a myriad of cognitive barriers (e.g., appropriate equipment sizes, drug doses) that make emergency airway management in neonates and children a source of significant anxiety.
Utilizing a systematic approach to airway management in young infants is paramount to success. This includes: (1) recognizing and addressing the predictable anatomic and physiologic differences in neonatal airway management, and (2) consistently applying an approach to airway management that identifies and addresses potential difficulties. In this chapter, we will review the most common presentations of neonatal patients requiring airway management in the ED, as well as provide a methodical approach to addressing both anticipated and unanticipated challenges that may occur.
Epidemiology and Experience
Opportunities to perform direct laryngoscopy and intubation are much less common in the pediatric than the adult population. It is estimated that airway management is required in 1–3 patients per 1,000 pediatric visits in the average ED compared with 6–10 intubations per 1,000 adult visits [10–12]. This number is further diluted when looking specifically at the care of young infants. The distribution of ages of patients requiring endotracheal intubation at a single tertiary care center for a 1-year period suggests that only a fraction of the pediatric population requiring airway management are neonates or young infants (Fig. 15). Given that the average ED physician will be unlikely to encounter opportunities for a significant number of pediatric airway procedures during typical clinical practice, skill acquisition, and retention can be difficult. Pediatric intubation success rates vary quite dramatically with experience. Studies performed in the operating room with anesthesia providers suggest that the success rate for endotracheal intubation after ten airways is less than 50 % while greater than 50 intubation attempts are required before success reaches 90 % [13, 14]. Therefore for emergency medicine providers with limited in situ clinical opportunities, the required number of intubations to attain “mastery” may therefore necessitate dedicated time in the operating room or augmentation of skills in a simulated environment [15].
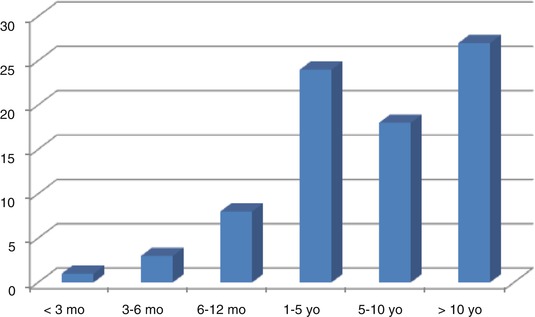
Fig. 15
Frequency of endotracheal intubation stratified by age
Pathophysiology
There are many unique anatomic and physiologic features that impact emergent neonatal airway management. These differences are predictable, and therefore can be anticipated and addressed to optimize early success and mitigate adverse events.
Anatomic differences in neonates compared to larger children or adults include relatively large occiputs compared with body size, a superior and anterior larynx, a large tongue relative to the oral cavity, a weaker hyoepiglottic ligament, and a large floppy epiglottis. The impact of each of these unique features on airway management, as well as the strategies to accommodate them is reviewed in Table 5.
Table 5
Addressing anatomic differences in children
Anatomic difference | Effect | Approach to management |
|---|---|---|
Large occiput | • Head flexion causes airway obstruction and limits glottic view | • Shoulder or neck roll to open airway and help align airway axes |
Superior/anterior larynx | • May limit glottic view | • Look up during laryngoscopy |
• Makes endotracheal tube delivery and passage difficult | ||
• Apply external laryngeal pressure | ||
• Create acute angle to styletted endotracheal tube | ||
Large tongue | • Falls onto posterior pharyngeal wall when supine obstructing airway | • Airway maneuvers or oral or nasal airway to open upper airway |
• Sweep the tongue when obstructing glottic view | ||
• May impede laryngoscopy | ||
Weak hyoepiglottic ligament | • Limits elevation of epiglottis through vallecular pressure | • Use straight laryngoscope blades
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|