Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

25

Use of Ophthalmic Laser in Children
 Corneal Laser Surgery
Corneal Laser Surgery
Excimer lasers used for corneal surgery are a relatively newly developed class of lasers with output in the ultraviolet range. The term excimer is derived from a contraction of “excited dimer.” An excited dimer is a reference to the electrically excited complex of a noble gas such as argon and a halide such as fluorine that occurs in the laser cavity. The wavelength of light is determined by the constituents of the dimer. The clinically most used excimer utilizes argon and fluorine to make up this dimer and produces 193-nm light. When the high-energy photons emitted strike the exposed corneal tissue, a unique interaction occurs, termed ablative photodecomposition. When this process occurs, molecular fragments are ejected from the surface at over 3000 m/s. There is little heat generated in this reaction and consequently almost none of the tissue distortion that is more typical of other laser tissue interactions.
 Laser Equipment
Laser Equipment
In the United States, three laser manufacturers have approval to market and sell their devices.
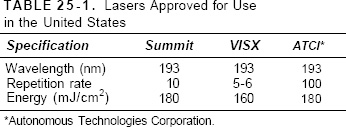
Table 25-1 lists the differences among the three approved lasers. Note that two of these lasers are wide-area ablaters and one is a spot scanner. The VISX system is illustrated in Figure 25-1. There are other types of lasers and delivery systems such as scanning slit and flying spot lasers. These other lasers are in various phases of the FDA approval process.
All calibration and centering procedures for each individual laser must be followed precisely to be sure that a beam of known energy and sufficiently high quality is delivered to the cornea. Typically, this calibration process requires ablating a material, such as a piece of plastic, and measuring the quantity of material ablated and the quality of the remaining cut. Each manufacturer has proprietary methods for calibration. Excimer lasers are more demanding in terms of maintenance than other lasers that ophthalmologists typically use (Fig. 25-2). As a result the technician who runs the machine has a very important role in its operation and calibration and is an integral member of the surgical team.
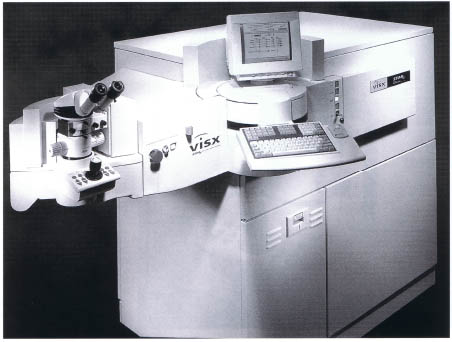
FIGURE 25-1. VISX STAR excimer laser system.
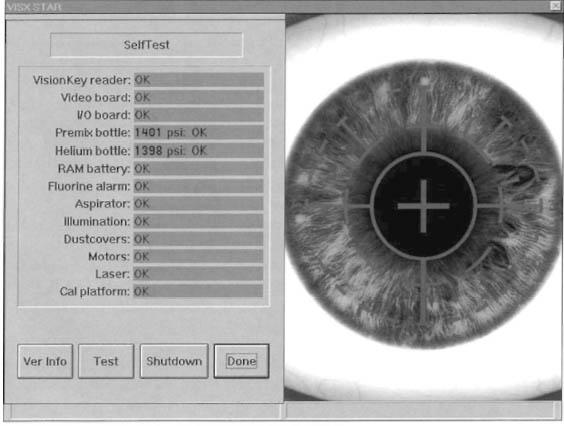
FIGURE 25-2. VISX STAR excimer laser system self-check.

FIGURE 25-3. Surgeon controls of the VISX STAR excimer laser system.
It is, however, the surgeon’s responsibility to ensure that all calibration and operating parameters are correct for the individual patient. Operating information including the desired treatment is entered into a computer, which contains the laser’s execution. Regardless of who enters the data into the computer (surgeon or technician), the operating surgeon is entirely and solely responsible for the patient’s treatment. This includes the verification of the data entered into the system for a particular treatment. The surgical parameters should be confirmed by the operating surgeon both visually and verbally prior to the initiation of any treatment (Fig. 25-3).
Specific Uses
These 193-nm excimer lasers are approved for the correction of scars and corneal irregularities (phototherapeutic keratectomy, PTK), the correction of mild to moderate myopia (photo refractive keratectomy [PRK]), the correction of mild to moderate myopia with concomitant astigmatism of between 0.75 and 4.0 diopters (PRKa), and the correction of high degrees of myopia (VISX only) and hyperopia (VISX only). However, none of these refractive modalities is approved for use in children in the United States. The minimum age for PRK to 6 diopters of myopia is 18 years, and for higher myopia and astigmatism (PRKa) it is 21 years. There is a recommended minimum age of 18 years for PTK, although there were patients treated in the clinical trials of these lasers who were less than 18 years and had obtained appropriate consent. There is, however, a growing body of international experience with these lasers in the pediatric population. This experience is entirely anecdotal with no prospective trials currently under way, although there is a university-based study soon to be started1,2 (E. Bluestein, M.D., personal communication). A second difficulty in describing the experience of children treated with the excimer laser is that it requires an extremely cooperative patient. The use of flammable anesthetics in and around this laser is specifically contraindicated. There are rare cases, however, where mask anesthesia or ketamine was used to temporarily immobilize the child outside of the laser suite, and then the essentially unconscious child is treated while in this “twilight” state.
There is very little published or reported about the use of the excimer laser to correct refractive errors in the pediatric population. Many surgeons are concerned about the developmental significance of Bowman’s layer, and its removal could precipitate a corneal ectasia. Laser in situ keratomileusis (LASIK) could also cause a similar ectasia through removal of stromal tissue and the near complete severing of Bowman’s layer, not to mention the added difficulty of placing the required instrumentation into a small, pediatric fissure. The peer-reviewed literature describes only two indications for PRK.
1. Anisometropia, which threatens to be amblyopiagenic, both hypermetropic and myopic.
2. Progressive and extreme myopia and refractive changes after pediatric cataract surgery.
Although not the only indications, these indications appear in the peer-reviewed literature. Administration of ketamine anesthesia is described in one of these reports for patients who are unable to cooperate with the treatment.
Results obtained thus far are very encouraging, with all patients reporting a reduction in refractive error. There is an improvement in best-corrected visual acuity in almost all patients. Significant haze is also reported, particularly in patients who are noncompliant with steroid regimens. The use of topical steroid medications in the pediatric population to prevent the formation of haze and subsequent visual acuity loss may be important. However, one should remember that this is only anecdotal information with very limited follow-up; that better study is warranted.
There were also pediatric patients treated in the United States under the PTK guidelines. These are patients who had posttraumatic scarring and leukoma, band keratopathy, or penetrating corneal trauma with a stepped wound.
Patients with Posttraumatic Scarring and Leukoma
Corneal trauma resulting in leukoma formation, which may be amblyopiagenic, can be effectively treated with the excimer laser. The principle behind any scar-reducing procedure is to remove as little tissue as possible to allow good vision. It is also important to avoid areas of corneal depression as the excimer laser removes and does not replace any tissue. The cornea does not need to be crystal clear to allow for the development of good visual acuity. It is important to reduce dense, confluent opacity to non-confluence. This will allow visual improvement while minimizing unwanted induced hyperopic or other refractive change (induced myopia or astigmatism). An important relationship exists between the diameter and depth of tissue ablated and the anticipated refractive change, even in a theoretically nonrefractive keratectomy such as PTK. Generally, the larger the diameter of tissue to be removed, the more tissue needs to be removed to effect a 1-diopter hyperopic shift. In normal (nonscarred) corneas, this translates to 12 [xm of tissue at a 6.0-mm diameter causing a 1-diopter shift, whereas at a 3.0-mm diameter this is only 3 μm per diopter. This relationship is for a refractive cut (PRK) and does not apply to the PTK-type cuts, although a similar yet nonlinear relationship appears to exist. Careful planning of tissue removal and avoiding hyperopic shifts from excessive tissue removal will allow the best clinical results.
One must be vigilant to ensure that leukoma formation in a pediatric patient is not caused by herpetic keratitis. A careful history and record review (where available) may alert the clinician to possible herpetic keratitis as a cause of leukoma formation. This is important because oral acyclovir prophylaxis has been shown to be effective controlling herpetic reactivations due to ultraviolet light in the adult population (the excimer lasers are intense sources of ultraviolet radiation). Additionally, topical antivirals are used over a 10- to 14-day taper period while the fresh epithelium closes the newly formed defect. One should not use the excimer laser to clear acute, active infections or inflammation (e.g., Thygeson’s and epidemic keratoconjunctivitis that are active). The laser expels tissue and does not necessarily destroy viral DNA; in fact, it may actually aerosolize these particles. It also causes a significant amount of inflammation in the healing of the keratectomy.
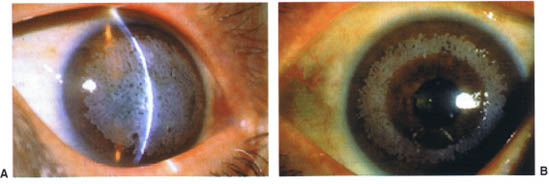
FIGURE 25-4. Calcific band keratopathy. (A) Preoperative. (B) Postoperative.
Band Keratopathy
If appropriately selected, patients with calcific band formation can be treated with the excimer laser (Fig. 25-4). Large, calcific changes are best handled with a chelation treatment or other manual debulking. However, feathery epithelial and subepithelial band formation can be removed quite easily with a very shallow transepithelial ablation. The principle of “less is better” also applies here. Patients must be carefully monitored at the slit lamp, if possible, during treatment. The cornea is not made completely clear, but rather the opacity is made nonconfluent so that the child will have better vision without unnecessary refractive shifts. It is important to recognize that the surgeon is, most likely, not curing the disease process but rather staving off amblyopia or making the child more comfortable to allow better vision. This process can be repeated several times on an eye as long as there is little or no stromal thinning.
Penetrating Corneal Trauma with a Stepped Wound
Following primary repair of laceration of the cornea (with or without tissue avulsion) in children, there can be an unevenness to the wound that does not occur in slower-healing, but comparable adult trauma. Once all the sutures are removed and the wound is deemed sufficiently stable (via refraction, keratometry, and/or videokeratography), one can ameliorate the corneal irregularity in one of any of a number of ways. The following are just two examples of these techniques:
1. A small spot size (1.5 to 2.0 mm) can be used in the PTK circle mode to smooth the scar and even the elevated spots, and a surface-modulating agent such as Tears Naturale II™ (0.3% methylcellulose) can be used to prevent ablation of depressed areas.
2. A slit sized to encompass the scar can be used to smooth and induce cylinder where appropriate (this variable slit mode is available on the VISX instrument as the PTK slit mode).
Both techniques are advanced and require a thorough understanding of optics and corneal responses and wound healing in pediatric patients. These techniques should only be undertaken by one well versed in the use of the excimer laser because the potential exists to worsen the problem through the induction of cylinder. A postoperative course of steroid and antibiotic is recommended to decrease chances of infection and corneal haze.
 Glaucoma
Glaucoma
Pediatric glaucoma broadly encompasses two types of disease: congenital glaucoma, which manifests and, it is hoped, is diagnosed within the first months of life, and infantile glaucoma, which becomes evident somewhat later in life, usually between ages 6 months and 1 year. Together these may be called developmental glaucomas. These glaucomas may be part of widespread syndromes, metabolic derangements, or localized abnormalities such as the phakomatoses (Sturge-Weber syndrome and neurofibromatosis). It is important to recognize the presence of a systemic condition both to institute possible treatment (e.g., dietary restriction in homocystinuria) and to understand the pathophysiology of the intraocular pressure abnormality (e.g., raised episcleral venous pressure in Sturge-Weber syndrome). Recognizing that there are various possible pathophysiological causes of intraocular pressure elevation in the pediatric population, one should also be aware that the vast majority of developmental glaucomas are open-angle glaucomas with some form of decreased outflow due to microscopic angle abnormality. The “congenital angle,” that is, the angle of patient with a developmental glaucoma, is variously described as being covered by a transparent membrane (Barkan’s membrane), having a high iris insertion, and having prominent iris processes, to name three of the more common descriptions. However it is described, the open angle and, more specifically, the trabecular meshwork (TM) are widely felt to be primary sites of disease in developmental glaucoma.
This knowledge allows us to understand why a particular laser application may or may not be appropriate. For example, laser iridotomies are rarely, if ever, performed primarily in developmental glaucoma because it is almost always an open angle form of glaucoma. Although it is true that some children develop iris bombe following intraocular surgery, even then laser iridotomy is rarely performed due to the inability of most infants and children to sit cooperatively at a laser with a goniolens coupled to their cornea. At most facilities, it is far easier to perform a surgical iridotomy in the operating room setting where general or mask anesthesia is administered than a laser iridotomy. Thus, laser iridotomy is not a procedure that is performed regularly in treating developmental glaucoma.
Laser trabeculoplasty (LTP), a mainstay in the treatment of adult open-angle glaucoma, is another procedure that is rarely used in the pediatric population. Knowing that developmental glaucoma is caused by an abnormal and sometimes poorly visible TM allows us to understand why LTP is not used in this setting. It is certainly impossible to treat the TM when there is a broad sheet of iris swept over the very structure targeted for LTP. The damage done to the iris and the secondary inflammation that is induced, which is usually quite exuberant in infants and children, make this procedure inappropriate in this group. Furthermore, in settings where the cornea is clear and the iris is not anteriorly inserted, it is questionable whether laser applications to the abnormal TM would have a beneficial effect. It is more likely that a paradoxical rise in intraocular pressure would result. The logistics of actually delivering a focused laser on the microscopic structure of a pediatric patient’s TM in the operating room setting (very different from the slit-lamp delivery systems normally used in adults) are also problematic.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


