Upper Airway Anatomy and Function
Gayle E. Woodson
The upper airway includes the nasal and oral cavities, the pharynx, and the larynx. The functional design is far from ideal because ingested food and water must traverse the upper airway to reach the alimentary tract. The pharynx must serve two conflicting functions. It must rapidly constrict to propel material into the esophagus during swallowing, yet maintain patency during the negative pressure generated by inspiration. The close proximity of the orifices into the esophagus and the lower airway present a significant risk of aspiration; therefore, the larynx has a major protective function, and breathing and speech must be interrupted during a swallow. The precarious arrangement of the airway is a product of its evolution and embryology. The trachea and lungs evolved as an offshoot of the digestive tract, and this origin is reflected in the development of human embryos. The lung buds arise from the lower pharynx.
In all nonhuman mammals, the common upper chamber for eating and breathing poses little problem, because there are functionally separate channels for breathing and eating, formed by the interdigitation of the epiglottis and the soft palate. The central channel, leading from the nose to the larynx, is for breathing, with a pathway for swallowing on either side, leading from the mouth to the esophagus. This configuration persists in human infants and explains why neonates experience such respiratory distress with nasal obstruction. In the second year of life, the larynx descends in the neck, associated with pharyngeal elongation, so that the soft palate and larynx are no longer in contact, but separated by a significant gap (1). This results in a larger hypopharyngeal space, which confers greater vocal power and diversity in articulation. But the separation of the uvula from the epiglottis abolishes the separation of air and alimentation pathways, which makes the process of swallowing considerably more complex. The purpose of this chapter is to provide the anatomic and physiologic basis for understanding the processes of breathing and speech. Because nasal and oral anatomy are covered in other parts of this text, the following section focuses primarily on the larynx and pharynx.
PHARYNGEAL ANATOMY
The pharynx is an irregularly tubular structure, extending from the base of the skull to the esophageal inlet (Fig. 61.1). The posterior and lateral walls of the pharynx are composed of three pharyngeal constrictor muscles attached to the cervical vertebrae posteriorly. The pharynx has anterior openings into the nasal and oral cavities, and inferiorly it opens into the larynx and esophagus. There are three segments: the nasopharynx, the oropharynx, and the hypopharynx. The nasopharynx can be sealed off from the oropharynx by simultaneous elevation of the soft palate and formation of a fold in the pharyngeal walls, known as Passavant ridge. Complete physical examination of the pharynx requires a mirror or endoscope, because only the posterior wall of the oropharynx is visible by transoral inspection.
The superior constrictor is suspended from the base of the skull, the medial pterygoid plate, the pterygomandibular raphe, the mylohyoid line of the mandible, and the lateral tongue. The anterior attachments of the middle constrictor are the hyoid bone and the stylohyoid ligament. The inferior constrictor attaches to the thyroid and cricoid cartilages. Activation of these muscles constricts the pharynx; there is no evidence to support the concept that they contribute to stability of the airway. Pharyngeal patency during the negative pressure generated with inspiration is maintained by muscles that dilate the lumen by pulling the base of the tongue or hyoid bone anteriorly. These muscles include the genioglossus, the geniohyoid, and the anterior belly of the digastric muscle.
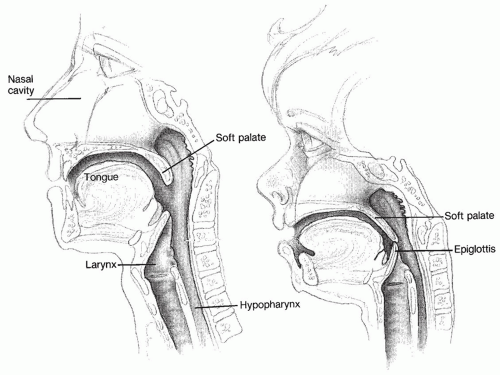 Figure 61.1 Sagittal view of upper airway. |
PHARYNGEAL AIRWAY PHYSIOLOGY
Maintenance of upper airway patency is a peculiarly human problem. Some degree of airway collapse occurs during sleep in all humans, and obstructive sleep apnea (OSA) is extremely common. But sleep disordered breathing is extremely rare in any other animal (2). The instability of the human pharyngeal airway is a byproduct of the inferior displacement of the larynx during development (3). The pharyngeal walls, suspended from the base of the skull and mandible, are pliable. Some skeletal support is provided by the hyoid bone. Because its walls are collapsible, the pharynx acts as a Starling resistor. Flow through such a resistor is not determined solely by the difference between the upstream and downstream (i.e., intrapleural) pressures, but is critically influenced by the difference between the upstream pressure and the collapsing forces. In other words, if the pressure of the air inspired through the nose is not high enough to keep the throat from collapsing, no air can reach the lungs, no matter how hard the inspiratory muscles contract, and obstructive apnea results. Snoring occurs when the collapsing pressure is less than upstream pressure, but greater than downstream pressure. The airway intermittently closes, but is reopened by increased upstream pressure (2).
As mentioned above, muscles that connect the hyoid bone and tongue base to the mandible provide the force to open the pharynx. These dilating muscles are activated by the negative airway pressure generated during inspiration in the presence of upper airway obstruction. During the Mueller maneuver, which generates negative pressure in the pharynx, the dilating muscles should maintain patency. A significant decrease in the cross-sectional area of the pharynx during the Mueller Maneuver is highly predictive of OSA (4). Thus, inadequate force of pharyngeal dilating muscles is implicated in the pathogenesis of OSA.
Patients with OSA have a higher than normal activity of phasic inspiratory activity of upper airway dilating muscles during wakefulness. This suggests that these individuals require more force than normal to keep the airway patent. They are able to compensate while awake, but during sleep, airway muscle activity decreases and is inadequate to prevent collapse during inspiration. Pharyngeal patency at end expiration is also a major factor. Endoscopic observations in patients with sleep apnea demonstrate a decrease in airway cross-sectional area before an actual obstructive event. At end-expiration, with no flow, the pharyx can collapse completely. When inspiration is attempted through an already obstructed airway, the result is an obstructive apnea. Continuous positive airway pressure can stent open the collapsed segment during end-expiration. This may be one mechanism by which continuous positive airway pressure (CPAP) therapy is effective. CPAP causes a decrease in genioglossus muscle activity during wakefulness in patients with sleep apnea, but not in normals, suggesting that the increased activity in the waking OSA syndrome patient represents compensation for a mechanically obstructed airway, not defective reflexes.
LARYNGEAL ANATOMY
The most superior portion of the larynx is the epiglottis, which projects posteriorly into the pharynx. The vallecula is the pouch between the base of the tongue and the epiglottis. Interiorly, the glottis is seen as a roughly triangular opening during inspiration and a narrow slit during phonation. The true vocal folds comprise the anterior edges of the glottis. Superior and lateral to the true vocal folds are the false vocal folds. The ventricle is a narrow space between the true and false folds. The posterior glottis is formed by the two arytenoid cartilages and the intervening mucosa. The arytenoids are the posterior attachments of both the true and false vocal folds. Opening and closing of the glottis is accomplished by action of muscles that move the arytenoids. There is a mucosal bridge between the epiglottis and the arytenoid on each side, known as the aryepiglottic fold. These folds serve as levees between the esophagus and airway, by separating the piriform fossae from the glottis. The piriform fossae are mucosal-lined spaces lateral to the aryepiglottic folds but medial to the laryngeal skeleton (Figs. 61.2, 61.3 and 61.4), and are the pathways by which ingested food and liquid are conveyed to the esophagus.
Skeleton
The laryngeal skeleton is made up of several cartilages and one bone strung together in series and suspended from the skull base and mandible (Fig. 61.5). Laryngeal motion can be caused by both intrinsic muscles, which arise and insert onto laryngeal cartilages, and extrinsic muscles, which connect the larynx to other structures. Also, descent of the trachea during inspiration produces widening of the glottis. This phenomenon is a result of the ligamentous interconnections of the laryngeal skeleton.
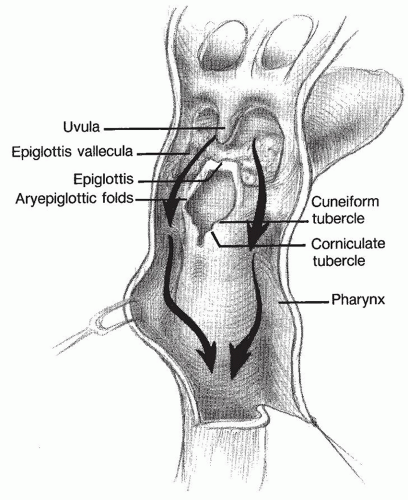 Figure 61.2 Posterior view of anterior airway. |
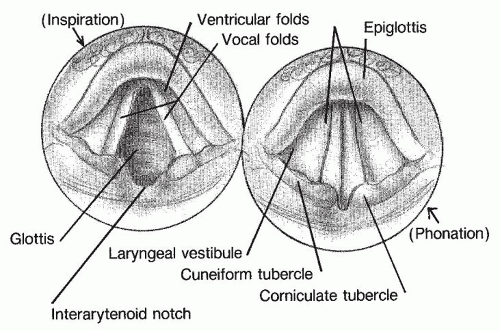 Figure 61.3 Endoscopic view of the larynx. |
The hyoid, which supports the larynx and stabilizes the hypopharynx, is roughly U shaped, with the two free ends projecting posteriorly as the greater cornua. The lesser cornua are two small bumps on the superior anterior surface. The hyoid is connected to the thyroid cartilage by the broad thyrohyoid membrane. A bursa in this membrane enhances vertical mobility of the larynx. Laterally, the edges of the membrane thicken to form the thyrohyoid ligaments.
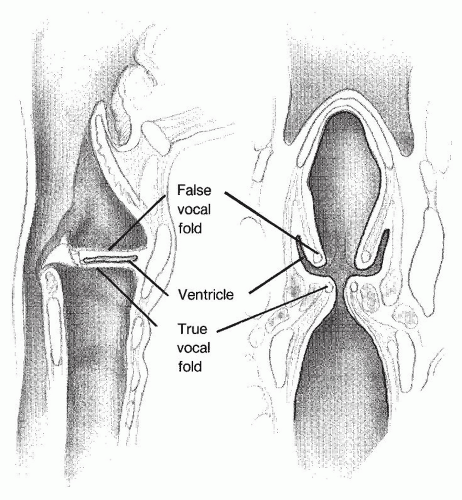 Figure 61.4 Vertical section through the larynx. |
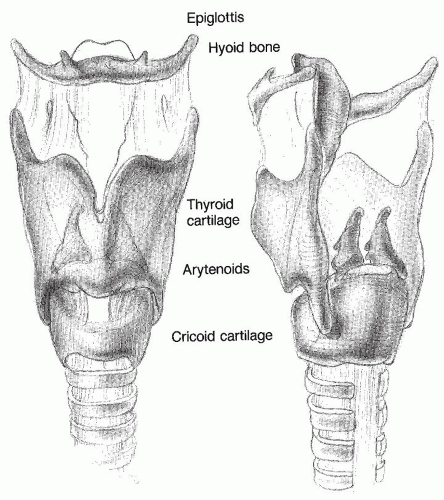 Figure 61.5 Laryngeal skeleton. |
The thyroid cartilage is composed of two halves fused anteriorly at a sharp angle (90 degrees in males and 120 degrees in females). The posterior border has superior and inferior cornua. The superior cornu attaches to the thyrohyoid ligament, whereas the inferior articulates with the cricoid cartilage. The thyroid cartilage begins to gradually ossify after the age of 20. This process accounts for many age-related changes in pitch and resonance of the voice.
The epiglottis is a fibroelastic cartilage, attached anteriorly in the midline to the inner surface of the thyroid cartilage and supported by the hyoepiglottic ligament. The free end of the epiglottis projects into the hypopharynx.
The cricoid cartilage is the skeletal support of the subglottis, which is the portion of the larynx below the vocal folds. The subglottis is the only point in the airway with a completely rigid diameter. It has a smaller crosssectional area than the trachea, so that a single foreign body that is small enough to pass through the subglottis does not cause total airway obstruction. Anteriorly, the cricoid is about 1 cm high, with a smooth curved surface. Posteriorly, it is 2 to 3 cm high, and the superior surface is flattened centrally to provide an area of articulation for the arytenoid cartilages. Posterolaterally, on each side, the cricoid articulates with the inferior cornu of the thyroid cartilage to form a visorlike apparatus, allowing rotation in a sagittal plane, which opens or closes the anterior cricothyroid space.
Each arytenoid cartilage is a somewhat pear-shaped mass. The broad base articulates with the cricoid in a complex synovial joint, which is essentially a shallow ball and socket, allowing multiaxial rotation but minimal translation (5). The vocal process, an anterior and medial projection of the arytenoid, is the posterior segment of the vocal fold (Fig. 61.6). Two other small sesamoid cartilages, the corniculate and the cuneiform, are located superior to the arytenoid and support the aryepiglottic fold.
Two fibroelastic membranes are important components of the larynx. The conus elasticus provides support to the vocal fold. From its lateral attachment to the cricoid, it extends anteriorly to the midline lower edge of the thyroid cartilage and posteriorly to the vocal process of the arytenoid. Its free edge forms the vocal ligament. The quadrangular membrane supports the supraglottis. It connects the epiglottis with the arytenoid and the corniculate cartilages. The superior free edge is draped in mucosa to form the aryepiglottic fold, whereas the inferior edge is a part of the false vocal fold (Fig. 61.7).
Muscles
Motion of the vocal folds is affected primarily by the intrinsic laryngeal muscles. It should be noted that each laryngeal muscle exerts a unique torque on the arytenoid. Physiologic motion results from the net effect of all muscles activated at any point in time (6). Thus, the vocal folds do not just open and close, but move in three-dimensional space and change shape.
The posterior cricoarytenoid muscle (PCA), the only abductor of the glottis, originates from the posterior surface of the cricoid and inserts onto the muscular process of the arytenoid. Contraction of this muscle externally rotates the arytenoid, displacing the vocal process superiorly and laterally, resulting in abduction of the glottis. However, the PCA is also activatated during phonation, presumably to stabilize the arytenoid and resist the anterior traction exerted by adductor muscles. Actually, the PCA consists of two compartments, which are innervated separately, and differ in fiber-type composition (7). The two compartments also differ in their action on the arytenoid. The horizontally oriented compartment causes rotation around a more vertical axis than does the oblique compartment (5




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
