Frontal Sinus Fractures
E. Bradley Strong
BACKGROUND
While frontal sinus injuries are relatively uncommon, the potential for long-term sequelae is significant. It is therefore critical to have a comprehensive treatment strategy. Unfortunately, optimal management of frontal sinus fractures remains controversial (1,2,3,4,5,6,7,8). Most authors would agree that a hierarchical treatment strategy would include: treatment of any intracranial injury, avoidance of short- and long-term complications such as mucoceles, reestablishment of an aesthetic facial contour, and return of normal sinus function if possible. This chapter provides an anatomically based treatment algorithm for the management of frontal sinus fractures, highlighting the key steps to surgical repair.
ANATOMY
The frontal sinus is not present at birth. The anterior ethmoid air cells invade the frontal bone at age 2; developing into a full size frontal sinus by age 15 (Fig. 84.1). The floor of the sinus forms the medial portion of the orbital roof. The posterior table forms a portion of the anterior cranial fossa. The anterior table forms part of the forehead, brow, and glabella (Fig. 84.2). The size and shape of the adult frontal sinus is highly variable. It is commonly asymmetric and may be divided by one or more septations. Less frequently, patients will have a unilateral (10%), rudimentary (5%), or no frontal sinus (4%). Average frontal sinus dimensions are: height 30 mm, width 25 mm, depth 19 mm, and volume 10 mL. The anterior table is much thicker (average 4 mm, but up to 12 mm) than the posterior table (0.1 to 5 mm) (9,10). The nasofrontal recess is the sole outflow tract for the frontal sinus. The ostia are approximately 1 to 3 mm in diameter and located posteriorly, inferiorly, and medially on the floor of the sinus (9,10). They are the narrowest point of an hourglass configuration, with the frontal sinus infundibulum above, and the nasofrontal recess below (Fig. 84.3).
PATHOPHYSIOLOGY
The frontal sinus is protected by thick cortical bone and is more resistant to fracture than any other facial bone (11) (Fig. 84.4). Consequently, frontal sinus fractures account for only 5% to 15% of maxillofacial injuries (1,11). The use of seat belts and airbags has significantly decreased the incidence of frontal sinus fractures (1,12). The majority of these fractures involve young males (average age 30 years) involved in high-velocity injuries such as motor vehicle accidents (52%), assaults (26%), and recreation or industrial accidents (14%) (1,5,6). Greater than 75% of patients will have associated facial fractures (1,7). Isolated anterior table fractures occur approximately 33% of the time. Combined fractures of the anterior table, posterior table, and/or the nasofrontal recess account for approximately 67% of frontal sinus injuries. Isolated posterior table injuries are rare (˜2% of injuries) (1,4).
DIAGNOSIS
Physical Examination
Due to the high velocity nature of these injuries, associated intracranial, spinal cord, thoracic, abdominal, and long bone injuries must be ruled out in all patients. A thorough history and complete head and neck examination are critical. Common physical findings include forehead abrasions/lacerations, contour irregularities, tenderness, paraesthesias, epistaxis, and hematoma. Exploration of forehead lacerations should be performed with sterile technique, if there is any question of intracranial violation. Through-and-through injuries of the frontal sinus have a high morbidity and prompt surgical treatment is indicated.
The presence of associated facial fractures must be ruled out, with special attention to examination of the orbits and nasoorbitoethmoid complex. Conscious patients should be questioned regarding the presence of watery rhinorrhea or salty tasting postnasal drainage suspicious for a cerebrospinal fluid leak. Such fluid should initially be evaluated with a “halo test.” The bloody fluid is allowed to drip onto filter paper. If cerebrospinal fluid is present, it will diffuse faster than blood and result in a clear halo around the blood. Beta-2 transferrin is the definitive test to confirm a cerebrospinal fluid leak; however, it is generally a “send out” test and may take 5 to 7 days to receive results.
The presence of associated facial fractures must be ruled out, with special attention to examination of the orbits and nasoorbitoethmoid complex. Conscious patients should be questioned regarding the presence of watery rhinorrhea or salty tasting postnasal drainage suspicious for a cerebrospinal fluid leak. Such fluid should initially be evaluated with a “halo test.” The bloody fluid is allowed to drip onto filter paper. If cerebrospinal fluid is present, it will diffuse faster than blood and result in a clear halo around the blood. Beta-2 transferrin is the definitive test to confirm a cerebrospinal fluid leak; however, it is generally a “send out” test and may take 5 to 7 days to receive results.
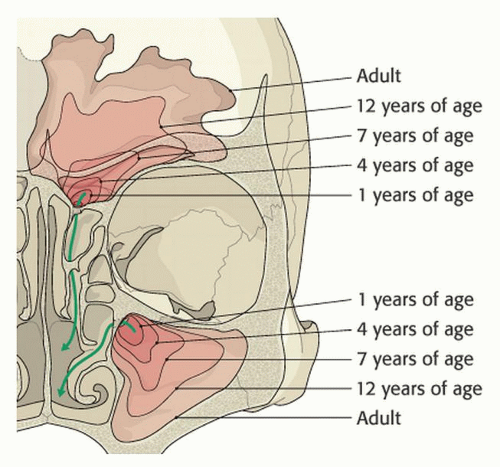 Figure 84.1 Frontal sinus development. The anterior ethmoid air cells invade the frontal bone at age 2. The sinus is fully developed by age 15. (From AO Surgery Reference Cranial Vault & Skull Base, www.aosurgery.org. Copyright by AO Foundation, Switzerland with permission). |
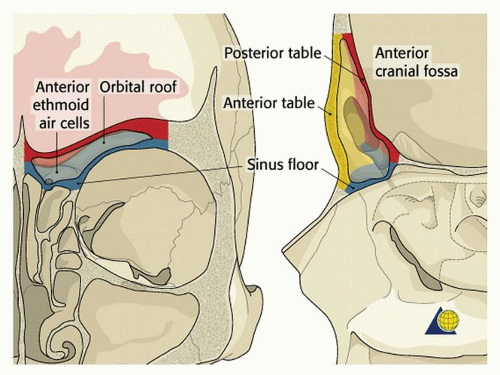 Figure 84.2 Frontal sinus anatomy. The anterior table of the frontal sinus is thick bone and provides forehead contour. The posterior table is thinner and constitutes a portion of the anterior cranial fossa. The floor or the sinus makes up a portion of the orbital roof. The frontal sinus ostia is located in the medial, posterior, and inferior portion of the sinus floor. (From AO Surgery Reference Cranial Vault & Skull Base, www.aosurgery.org. Copyright by AO Foundation, Switzerland with permission). |
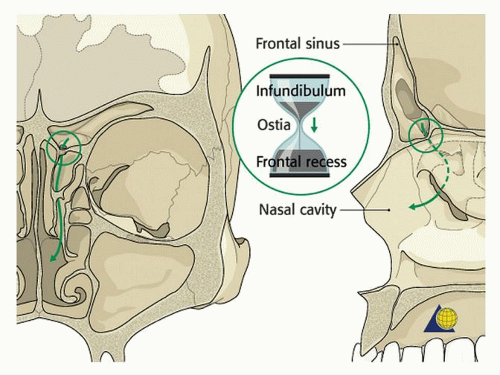 Figure 84.3 Frontal sinus drainage. The frontal sinus drainage pathway has an hourglass configuration with the infundibulum above and the frontal recess below. (From AO Surgery Reference Cranial Vault & Skull Base, www.aosurgery.org. Copyright by AO Foundation, Switzerland with permission). |
Radiography
Plain radiographs are of little use in the diagnosis of frontal sinus fractures. A thin cut (1.0 to 1.5 mm), axial computed tomography (CT) scan is the gold standard. It is recommended to obtain coronal, sagittal, and three-dimensional (3-D) reconstructions for diagnostic accuracy. The axial images are used to evaluate the anterior and posterior tables (Fig. 84.5); coronal images for the sinus floor and orbital roof (Fig. 84.6). Sagittal images can be useful in assessing the patency of the frontal recess (Fig. 84.7) (13), while 3-D reconstructions help define the shape, location, and orientation of individual bone fragments that are seen less clearly on 2-D views (Fig. 84.8). The 3-D information can reduce the need for surgical dissection, because the surgeon knows the number, location, and orientation of the larger bone fragments. It can also help the patient and/or family to understand the bony anatomy and severity of the injury.
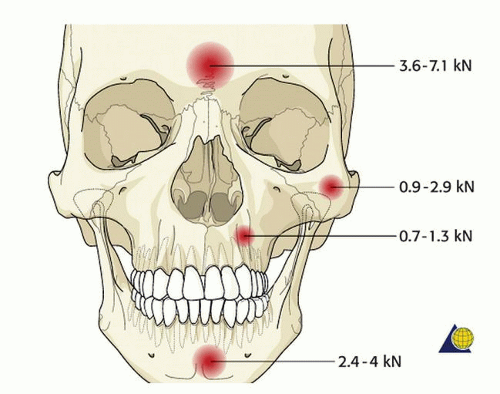 Figure 84.4 The anterior table of the frontal sinus is thick cortical bone. It is more resistant to fracture than any other facial bone. (From AO Surgery Reference Cranial Vault & Skull Base, www.aosurgery.org. Copyright by AO Foundation, Switzerland with permission). |
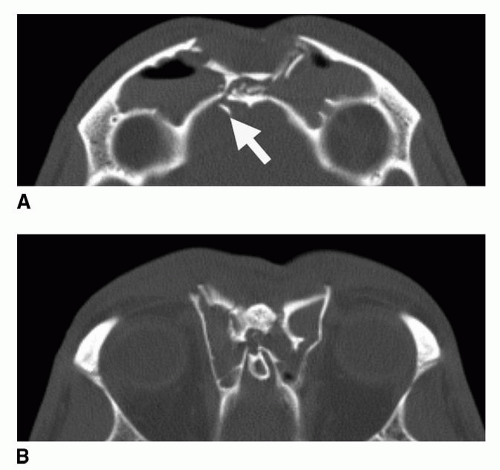 Figure 84.5 Axial CT scan demonstrating a frontal sinus fracture involving both the anterior and posterior tables. A: Marked anterior table disruption. The white arrow points out a displaced posterior table bone fragment. B: Disruption of the nasofrontal recess. (From Strong, EB. Frontal sinus fractures: current concepts. Craniomaxillofac Trauma Reconstr 2009;2(3):161-175, figure 2.) |
TREATMENT ALGORITHM
The appropriate treatment strategy for the management of frontal sinus fractures can be made by assessing four anatomic parameters (Fig. 84.9). These parameters include the presence of: (a) an anterior table fracture, (b) a posterior table fracture, (c) a nasofrontal recess fracture, (d) a dural tear (cerebrospinal fluid leak). These findings can be applied to the algorithm presented to determine appropriate treatment (Table 84.1). The treatment options include: observation, endoscopic repair, open reduction and internal fixation, sinus obliteration, sinus cranialization, and rarely sinus ablation (Reidel procedure). The indications and techniques for each of these procedures are discussed below.
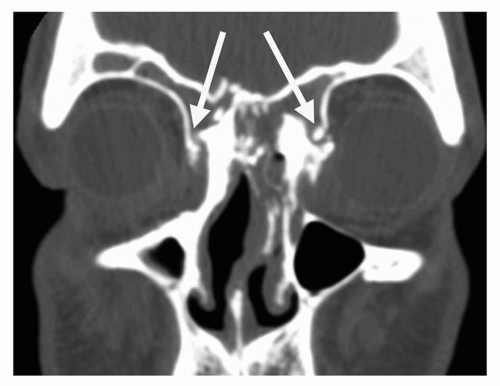 Figure 84.6 Coronal CT scan demonstrating disruption of the medial orbit and frontal recess (arrows). (From Strong, EB. Frontal sinus fractures: current concepts. Craniomaxillofac Trauma Reconstr 2009;2(3):161-175, figure 3.) |
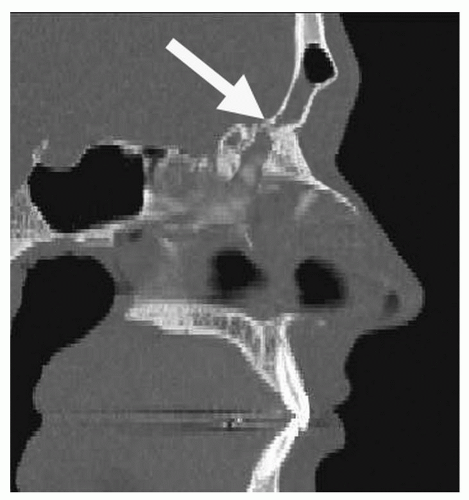 Figure 84.7 Sagittal CT scan demonstrating a frontal sinus fracture. The arrow demonstrates narrowing and obstruction of the frontal sinus outflow tract. (From Strong, EB. Frontal sinus fractures: current concepts. Craniomaxillofac Trauma Reconstr 2009;2(3):161-175, figure 4.) |
Frontal Recess Fractures
Frontal recess fractures result in disruption of the sole frontal sinus outflow tract (Fig. 84.10 and Table 84.1). Frontal recess
fractures that result in sinus outflow obstruction will generally require frontal sinus obliteration. Unfortunately, the compact anatomy of the frontal recess makes accurate diagnosis challenging. One option is to perform a frontal sinus trephination to visualize the recess endoscopically. This does, however, require a general anesthetic. Some authors have proposed infusion of dye into the sinus to document frontal recess patency. Unfortunately, the passage of dye into the nose does not confirm or refute the presence of a fracture and has no documented prognostic value for the ultimate patency of the frontal recess. Therefore treatment decisions are generally based on thin cut CT scans. If the frontal recess patency remains in question (and there are no other significant sinus injuries) patients may be followed with sequential CT scans at approximately 1 and 12 months to assure that the frontal recess is patent. If the frontal recess becomes obstructed an obliteration is indicated. A more recently described technique involves observation of limited frontal sinus fractures (with serial CT scans), followed by endoscopic frontal sinusotomy for management of frontal recess stenosis (14). While
this approach shows some promise, it should be reserved for surgeons with extensive experience in both endoscopic sinus surgery as well as open approaches to the frontal sinus.
fractures that result in sinus outflow obstruction will generally require frontal sinus obliteration. Unfortunately, the compact anatomy of the frontal recess makes accurate diagnosis challenging. One option is to perform a frontal sinus trephination to visualize the recess endoscopically. This does, however, require a general anesthetic. Some authors have proposed infusion of dye into the sinus to document frontal recess patency. Unfortunately, the passage of dye into the nose does not confirm or refute the presence of a fracture and has no documented prognostic value for the ultimate patency of the frontal recess. Therefore treatment decisions are generally based on thin cut CT scans. If the frontal recess patency remains in question (and there are no other significant sinus injuries) patients may be followed with sequential CT scans at approximately 1 and 12 months to assure that the frontal recess is patent. If the frontal recess becomes obstructed an obliteration is indicated. A more recently described technique involves observation of limited frontal sinus fractures (with serial CT scans), followed by endoscopic frontal sinusotomy for management of frontal recess stenosis (14). While
this approach shows some promise, it should be reserved for surgeons with extensive experience in both endoscopic sinus surgery as well as open approaches to the frontal sinus.
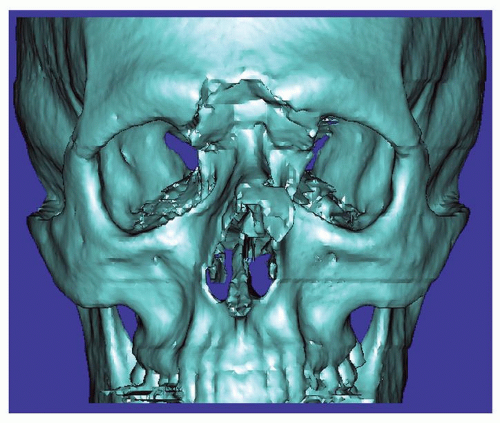 Figure 84.8 3-D CT scan of a frontal sinus fracture. The 3-D reconstruction can be helpful in delineating the position of bone fragments to be located intraoperatively. (From Strong, EB. Frontal sinus fractures: current concepts. Craniomaxillofac Trauma Reconstr 2009;2(3):161-175, figure 5.) |
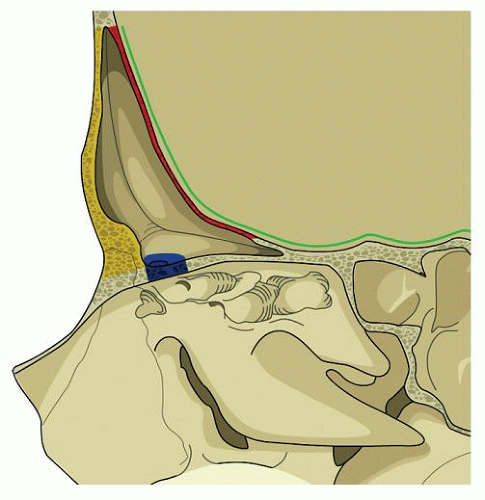 Figure 84.9 Illustration of the anatomic parameters that need to be assessed when developing a treatment plan for frontal sinus fractures. Yellow—anterior table; Red—posterior table; Blue— frontal recess; Green—dural integrity. (From Strong, EB. Frontal sinus fractures: current concepts. Craniomaxillofac Trauma Reconstr 2009;2(3):161-175, figure 6.) |
TABLE 84.1 FRONTAL SINUS FRACTURES | |
|---|---|
|
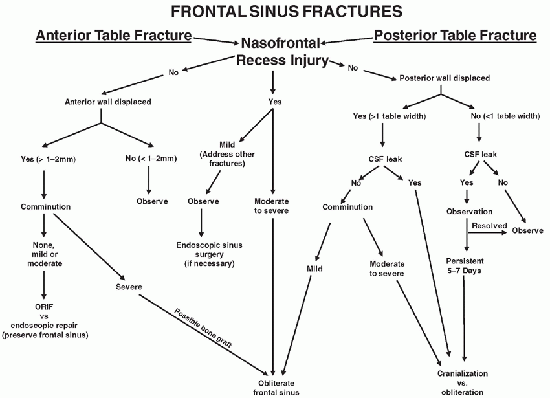
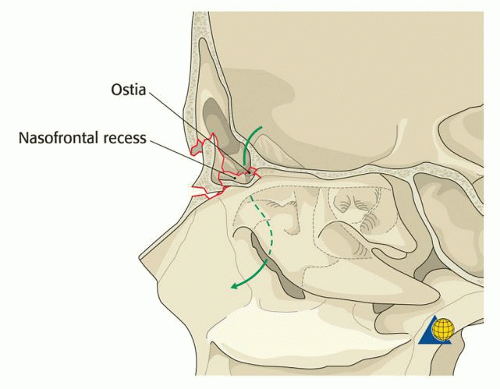 Figure 84.10 Illustration of frontal recess fracture—the sole outflow tract of the frontal sinus. (From AO Surgery Reference Cranial Vault & Skull Base, www.aosurgery.org. Copyright by AO Foundation, Switzerland with permission). |
Anterior Table Fractures
Nondisplaced (0 to 2 mm) anterior table fractures can be observed with little risk of long-term morbidity (Fig. 84.11 and Table 84.1). Fractures with greater displacement (2 to 6 mm) present little risk of mucocele formation; however, the risk of an aesthetic deformity increases with the degree of displacement (Fig. 84.12). In these situations, the decision for an open reduction should not be based on the long-term risk of sinusitis/mucocele formation. Most sinuses will heal adequately. The decision for surgery should be carefully weighed against the risks of general anesthesia and the long-term iatrogenic sequelae from a coronal incision (i.e., alopecia, paresthesias, facial nerve injury, etc.). Historically, these sequelae have been downplayed, but they can be more severe than the injury itself. Alternatively, minimally invasive approaches may be indicated with mildly displaced fractures. Transcutaneous upper eyelid approaches have been described, but have not gained significant popularity (15,16). Endoscopic fracture reduction in the acute setting has also been described, but is technically challenging (17,18,19,20,21). The author feels it is not a viable technique for the majority of patients. Therefore, if an endoscopic approach is chosen, the author prefers a camouflage technique (17,18,20). Surgery for camouflage of the external deformities is performed 2 to 3 months after the injury when all facial swelling has resolved. This allows the patient to assess the degree of deformity and make an accurate decision as to whether they desire surgical intervention. Patients with thicker skin are better candidates for this approach because any subtle defects will be more easily camouflaged. If the patient is seen acutely, the rationale and indications for a delayed approach must be clearly explained (i.e., risk of iatrogenic injury may be greater than the traumatic deformity itself); and the patient must understand that a fracture reduction cannot be performed once the fracture has healed. While the risk of mucocele formation is very low, this should also be discussed. In the author’s experience, many patients with minimally displaced fractures will desire no surgical intervention due to the lack of significant deformity. More complex anterior table fractures (greater than 6 mm or with comminution) will likely require open reduction using a coronal incision (Fig. 84.13). Uncommonly frontal sinus obliteration may be required when severe mucosal injuries are present.
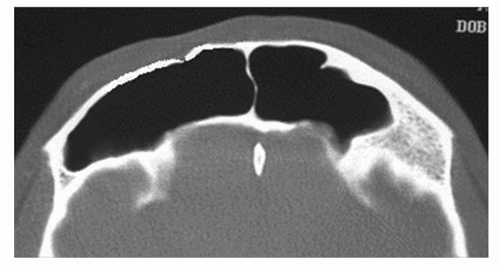 Figure 84.11 Axial CT scan demonstrating a minimally displaced anterior table fracture. These injuries have a low risk of mucocele formation or aesthetic deformity. |
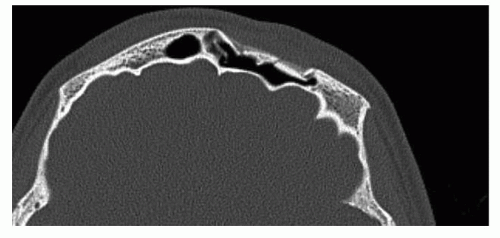 Figure 84.12 Axial CT scan demonstrating a mild to moderately displaced anterior table fracture. These fractures have a more significant risk of long-term aesthetic deformity. |
Posterior Table Fractures
The treatment algorithm for posterior table fractures is complex due to the risk of CSF leak, meningitis, and mucocele formation (Table 84.1) (2,4,5




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
