Purpose
To analyze the uncorrected binocular performance after biaspheric multifocal central presbyopic laser in situ keratomileusis treatments.
Design
Retrospective, interventional case series.
Methods
setting . Private clinical practice. patient or study population . Three hundred fifty-eight presbyopic patients (43% males, 82 myopic), bilaterally treated, suitable for laser in situ keratomileusis, with monocular corrected distance visual acuity of 20/32 or better. intervention or observation procedure(s) . PresbyMAX (Schwind Eye-Tech-Solutions GmbH and Co) biaspheric multifocal ablation. main outcome measures . Binocular uncorrected distance visual acuity (UDVA) and near visual acuity (UNVA) after surgery and their changes compared with corrected distance visual acuity and corrected near visual acuity before surgery.
Results
At 6 months, 76% of patients achieved a UDVA of 0.1 logarithm of the minimal angle of resolution (logMAR; Snellen equivalent, 20/25) or better, 91% of patients obtained a UNVA of 0.1 logarithmic of the reading acuity determination (logRAD) (p3) or better, and 99% of patients were within 1 diopter of defocus. Postoperative mean spherical equivalent was −0.17 ± 0.34 diopter. Ninety-six percent of patients achieved a UDVA of 0.2 logMAR (Snellen equivalent, 20/32) or better and a UNVA of 0.2 logRAD (p4) or better. Mean binocular corrected distance visual acuity degraded from 0.00 ± 0.01 logMAR (Snellen equivalent, 20/20) to a UDVA of 0.09 ± 0.07 logMAR (Snellen equivalent, 20/25). Mean binocular corrected near visual acuity degraded from 0.02 ± 0.01 logRAD (p2) to a UNVA of 0.07 ± 0.07 logRAD (p2).
Conclusions
Although optically the results are predictable, approximately 17% of the patients did not obtain objectively successful outcomes. In presbyopic patients without symptomatic cataracts, but with refractive errors, the PresbyMAX will decrease the presbyopic symptoms and correct far distance refraction in the same treatment, offering spectacle-free vision in daily life in most of the patients. Further investigation is necessary to evaluate the overall benefit of this procedure.
Refractive corrections for presbyopia by excimer laser systems are as old as laser refractive surgery itself. Vinciguerra and associates proposed a 10 to 17-μm deep semilunar-shaped zone immediately below the pupillary center, steepening the corneal curvature in that area, and reported promising results with this technique.
Monovision is another extended technique, usually in the form of dominant eye correction for distance as opposed to crossed monovision (dominant eye corrected for near), offering better near vision than that of control patients. Attempts for pseudoaccommodative cornea opened new concepts for correction of presbyopia in the form of a peripheral near zone (concentric ring for near vision) or in the form of a central near zone (central disc for near vision).
Ortiz and associates characterized the optical quality by the Strehl ratio, the spot size on the retina, and objective decimal visual acuity calculated based on measured corneal topography using the Fresnel propagation algorithm based on a realistic eye model. They found that with a complete characterization of the eye and a complete propagation algorithm (that takes into account all refractive surfaces in the eye at the same time), it is possible to evaluate the optical quality in eyes of patients who have undergone central presbyopic laser in situ keratomileusis (presbyLASIK) treatment. Reinstein and associates successfully combined extended depth of focus with monovision in a micromonovision protocol, whereas Epstein and Gurgos combined monocular peripheral presbyLASIK in the nondominant eye with monofocal distance correction in the dominant eye.
Few studies exist examining binocular uncorrected performance after presbyLASIK compared with binocular best-corrected performance before surgery (ie, uncorrected perception of the patient compared with the best experience before surgery). The purpose of this study was to investigate the uncorrected binocular performance (distance and near) 6 months after a biaspheric multifocal central presbyLASIK approach called PresbyMAX (Schwind Eye-Tech-Solutions GmbH and Co. KG, Kleinostheim, Germany) based on the creation of a biaspheric, multifocal corneal surface with a multifocal central area for near vision correction surrounded by an area where ablation is calculated for distance emmetropia treatments for myopia and hyperopia with or without astigmatism.
Methods
This was a retrospective, interventional case series. There was no institutional review board or ethical committee review and approval of this study. This was an interventional study, but it was not using investigational treatments on human subjects. It was evaluating the use of software, which bears CE mark as medical device, and the treatments were not investigational in Europe.
Patient Selection
Patients were enrolled in the study if they were presbyopic, were medically suitable for LASIK, had best-corrected distance visual acuity (CDVA) of 20/32 or better in both eyes using the Early Treatment Diabetic Retinopathy Study chart, demonstrated stable refraction for 1 year before the study, and discontinued contact lenses for at least 2 to 4 weeks (depending on contact lens type) before the preoperative evaluation. A line of CDVA or uncorrected distance visual acuity (UDVA) was deemed read if 3 of 5 letters of that line were recognized correctly.
Patients were required to have normal keratometry and topography results and to complete a minimum follow-up of 6 months. Patients had to have pupil diameters smaller than 3.0 mm in photopic high conditions and more than 4.5 mm in mesopic low conditions to be included.
Patients with a systemic illness, who had a calculated postoperative corneal bed thickness of less than 300 μm after ablation, who had preoperative central corneal thickness of less than 500 μm, who had undergone previous ocular surgery, or who had abnormal corneal topography were excluded from the study. Additional exclusion criteria were clinically relevant lens opacity, an ectopic pupil more than 1 mm off center, and any signs of binocular vision anomalies at distance and near.
Informed consent and permission to use the patient’s data for analysis and publication were obtained from each patient. Seven hundred sixteen eyes of 358 patients (43% males and 82 myopic patients) undergoing bilateral LASIK for refractive presbyopic corrections were enrolled. The average age was 53 ± 6 years (range, 41 to 67 years; Table 1 ). Mean preoperative spherical equivalent (SE) was 0.42 ± 2.44 diopters (D; range, −9.25 to 4.75 D; median, 1.25 D). Mean preoperative astigmatism was 0.48 ± 0.59 D (range, 0.00 to 5.00 D; median, 0.50 D), and mean spectacle near addition was 2.04 ± 0.43 D (range, 1.00 to 2.75 D; median, 2.00 D).
| Age Group (y) | Myopes (n = 82 Patients), % | Hyperopes (n = 276 Patients), % |
|---|---|---|
| 41 to 45 | 11 | 7 |
| 46 to 50 | 32 | 25 |
| 51 to 55 | 35 | 30 |
| 56 to 60 | 17 | 23 |
| 61 to 65 | 5 | 15 |
Preoperative Assessment
A full ophthalmologic examination was performed on all patients before surgery, including manifest refraction, cycloplegic refraction, slit-lamp microscopy of the anterior segment, dilated funduscopy, and Goldmann intraocular pressure measurement. The preoperative examination also included topography, keratometry, and pupillometry (Scout; Optikon, Rome, Italy) and handheld ultrasound pachymetry (Corneo-Gage Plus; Sonogage, Cleveland, Ohio, USA). Uncorrected near visual acuity (UNVA), distance corrected near visual acuity (DCNVA), and corrected near visual acuity (CNVA) were assessed with Parinaud reading charts at 33 cm.
Surgical Procedure
All treatments were prepared using the Schwind PresbyMAX treatment planning module in the aspheric mode (CAM software version 4.3; Schwind Eye-Tech-Solutions GmbH and Co. KG). This module integrates biaspheric multifocal ablation profiles combining 2 focus-shifted aspheric profiles with different asphericities that compensate as well for the peripheral loss of energy resulting from an increased angle of incidence on the cornea. The treatment of ocular or corneal wavefront aberrations was not intended in this study.
In this presbyopic concept, both eyes equally contribute to providing visual acuity at all distances by actively participating in the visual process for creating binocular vision impressions. The sphere and cylinder values entered into the laser were based on the manifest refraction without nomogram adjustment. The addition was overplanned by 0.50 to 0.75 D to ensure inducement of multifocality (2.68 ± 0.42 D; range, 1.50 to 3.50 D; median, 2.75 D).
Optical treatment zone diameters were 6.47 ± 0.16 mm (range, 5.8 to 7.0 mm; median, 6.5 mm). For each treatment, the planning software calculated the size of the transition zone, depending on the preoperative refraction and optical zone. The total ablation zone ranged from 6.6 to 8.9 mm.
The surgical procedure is the same as that for standard LASIK treatments with the AMARIS (Schwind Eye-Tech-Solutions GmbH and Co. KG). Flaps were created with a Carriazo-Pendular microkeratome (Schwind Eye-Tech-Solutions GmbH and Co. KG) using 110- or 130-μm heads (nominal flap thickness). Both the flap and the ablation profile were centered on the corneal vertex determined at the topographer, which closely approximates the visual axis.
Postoperative Evaluation
Patients were reviewed at 1 day, 1 month, 3 months, and 6 months after surgery. All postoperative follow-up visits included measurement of monocular and binocular UDVA and UNVA. Manifest refraction and CDVA, DCNVA, and CNVA were obtained at all postoperative visits after the day 1 appointment. Scout topography was performed at the 3- and 6-month visits.
Outcome Measures
Binocular uncorrected distance and near visual acuities
Outcome measure included postoperative mean values and ranges as well as change from preoperative binocular CDVA and CNVA; histogram distributions; univariate correlations of the changes from preoperative binocular CDVA and CNVA with the planned refraction, addition, optical zone, and age; and the respective cutoff values (additions and refraction that lead to a loss of 1 line of binocular CDVA or CNVA).
Binocular uncorrected distance versus near visual acuities
We determined binocular success as a UDVA of 0.15 logarithm of the minimal angle of resolution (logMAR; Snellen equivalent, 20/28) or better and a UNVA of 0.15 logRAD (p3) or better. We determined the correlation between binocular UDVA and binocular UNVA.
Accuracy
Scattergram for SE refraction at the 6-month follow-up was plotted. The refractive deviation from target for distance correction was evaluated in SE and astigmatism.
Statistical Analyses
The differences in refractive outcomes and visual acuities before and after surgery were evaluated using the paired Student t test. Scattergrams were assessed using the coefficient of determination ( r 2 ); the significance of the correlations was evaluated considering a metric distributed approximately as a t statistic with N − 2 degrees of freedom, where N is the size of the sample. A P value less than .05 was considered statistically significant.
Results
Preoperative Results
For myopes, binocular CDVA averaged 0.01 ± 0.02 logMAR (Snellen equivalent, 20/20) and ranged from 0.0 to 0.1 logMAR (Snellen equivalent, 20/20 to 20/25), whereas binocular CNVA averaged 0.02 ± 0.01 logRAD (p1.9) and ranged from 0.0 to 0.1 logRAD (p1.7 to p2.7).
For hyperopes, binocular CDVA averaged 0.00 ± 0.01 logMAR (Snellen equivalent, 20/20) and ranged from 0.0 to 0.1 logMAR (Snellen equivalent, 20/20 to 20/25), whereas binocular CNVA averaged 0.02 ± 0.01 logRAD (p1.9) and ranged from 0.0 to 0.1 logRAD (p1.7 to p2.7).
Postoperative Results at 6-Month Follow-Up
Binocular uncorrected distance visual acuity
For myopes, UDVA averaged 0.10 ± 0.08 logMAR (Snellen equivalent, 20/25) and ranged from 0.0 to 0.4 logMAR (Snellen equivalent, 20/20 to 20/50). The change in UDVA compared with preoperative CDVA was statistically significant ( P < .0001), with a mean difference of −1.0 ± 0.7 lines (range, −4 to 0 lines; median, −1 lines). UDVA was 20/32 or better in 80 (98%) patients ( Figure 1 , Top). Twenty-two (27%) patients achieved a UDVA of 2 lines or more lower than the preoperative CDVA ( Figure 2 , Top).
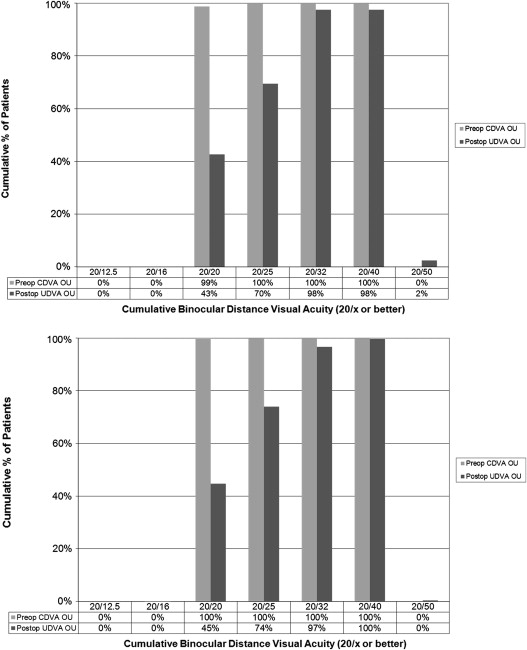
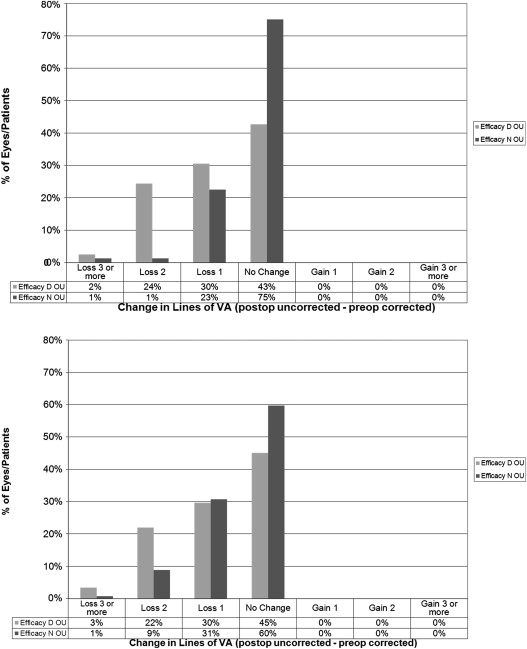
For hyperopes, UDVA averaged 0.09 ± 0.08 logMAR (Snellen equivalent, 20/25) and ranged from 0.0 to 0.4 logMAR (Snellen equivalent, 20/20 to 20/50). The change in UDVA compared with preoperative CDVA was statistically significant ( P < .0001), with a mean difference of −0.9 ± 0.7 lines (range, −4 to 0 lines; median, −1 lines). UDVA was 20/32 or better in 269 (97%) patients ( Figure 1 , Bottom). Sixty-eight patients (25%) patients obtained a UDVA of 2 lines or more lower than the preoperative CDVA ( Figure 2 , Bottom).
Univariate correlations of the changes (in lines) in UDVA compared with the preoperative CDVA showed statistically significant correlations with the planned addition ( P < .0001; with a slope of −0.59 and an intercept of 0.71 lines) and age ( P < .0001; with a slope of −0.03 and an intercept of 0.98 lines), and the cutoff values were 2.88 D for the planned addition (higher planned additions lead to a UDVA lower than the preoperative CDVA) and 58 years for age (older patients lead to a UDVA lower than the preoperative CDVA).
Binocular uncorrected near visual acuity
For myopes, UNVA averaged 0.05 ± 0.06 logRAD (p2.2) and ranged from 0.0 to 0.3 logRAD (p1.5 to p5.3). The change in UNVA compared with preoperative CNVA was statistically significant ( P < .0001), with a mean difference of −0.3 ± 0.6 lines (range, −3 to 0 lines; median, 0 lines). UNVA was p3 or better in 98% of patients ( Figure 3 , Top). Two percent of patients obtained a UNVA of 2 lines or more lower than the preoperative CNVA ( Figure 2 , Top).
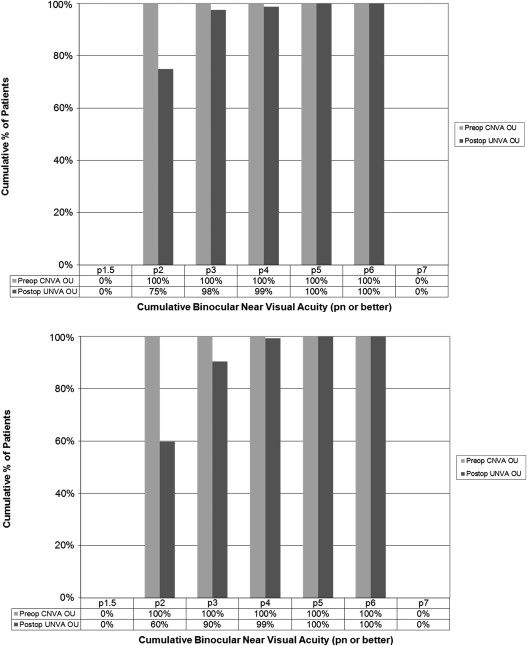
For hyperopes, UNVA averaged 0.08 ± 0.07 logRAD (p2.5) and ranged from 0.0 to 0.3 logRAD (p1.5 to p5.3). The change in UNVA compared with preoperative CNVA was statistically significant ( P < .0001), with a mean difference of −0.5 ± 0.7 lines (range, −3 to 0 lines; median, 0 lines). UNVA was p3 or better in 90% of patients ( Figure 3 , Bottom). Ten percent of patients obtained a UNVA of 2 lines or more lower than the preoperative CNVA ( Figure 2 , Bottom).
Univariate correlations of the changes (in lines) in UNVA compared with preoperative CNVA with the planned refraction, addition, optical zone, and age showed no statistically significance.
Binocular uncorrected distance versus near visual acuities
For myopes, simultaneous distance and near vision of 20/25 UDVA and p3 UNVA was achieved in 55 (67%) patients, whereas 20/32 CDVA and p4 was achieved in 79 (96%) patients ( Figure 4 , Top). We determined binocular success as a UDVA of 0.15 logMAR (Snellen equivalent, 20/28) or better and a UNVA of 0.15 logRAD (p3) or better. According to these limits, 72 (88%) patients achieved binocular success under uncorrected conditions.
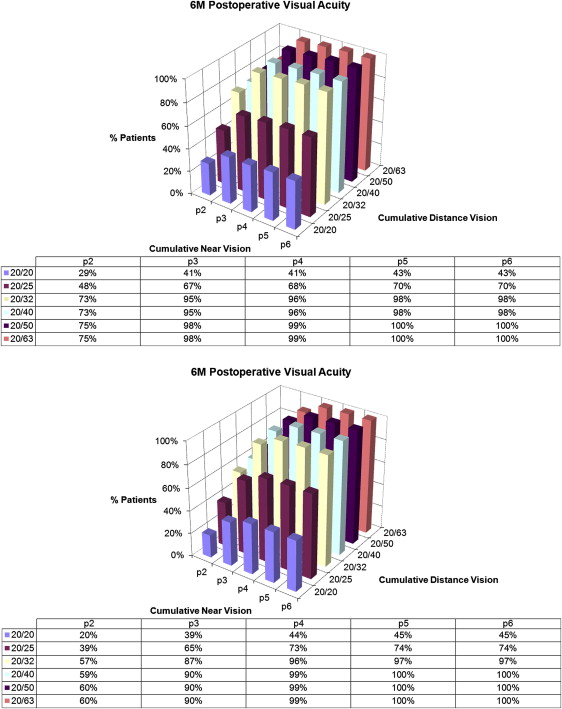
For hyperopes, simultaneous distance and near vision of 20/25 UDVA and p3 UNVA was achieved in 180 (65%) patients, whereas 20/32 CDVA and p4 was achieved in 266 (96%) of the patients ( Figure 4 , Bottom). We determined binocular success as a UDVA of 0.15 logMAR (Snellen equivalent, 20/28) or better and a UNVA of 0.15 logRAD (p3) or better. According to these limits, 222 (80%) patients achieved binocular success under uncorrected conditions.
We determined the correlation between UDVA and UNVA to be statistically significant ( P < .001; with a slope of −0.26 and an intercept of −0.72 lines, that is, the lower the UNVA compared with preoperative CNVA, the higher the UDVA compared with preoperative CDVA, but in a rate of 3.8:1).
We defined a metric of success of the form:
For myopes, global loss averaged −0.8 ± 0.5 lines and ranged from −2 to 0 lines, whereas for hyperopes, global loss averaged −0.9 ± 0.5 lines and ranged from −3 to 0 lines. Univariate correlations of the global loss showed statistically significant correlations with the planned addition ( P < .0001; with a slope of −0.31 and an intercept of −0.03 lines) and age ( P < .0001; with a slope of −0.03 and an intercept of 0.64 lines), and the cutoff values were 3.10 D for the planned addition (higher planned additions represent a relevant global loss) and 58 years for age (older patients represent a relevant global loss).
Accuracy
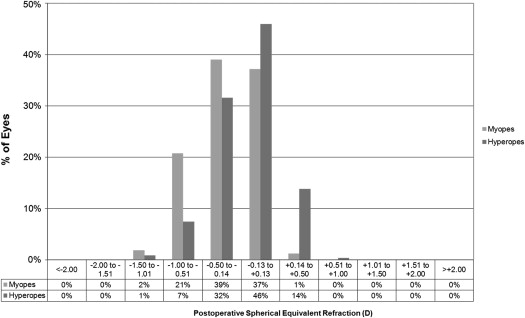
Figures 5 and 6 show a histogram of the accuracy of the SE and astigmatic correction, respectively. Figure 7 shows a scattergram of the achieved versus attempted refractive correction for SE.