Purpose
To investigate the retention rate and complications of 2 different types of silicon lacrimal punctal plugs with the focus on the relationship to punctum size.
Design
A prospective, nonrandomized, interventional, comparative study.
Method
Forty-four patients with dry eye syndrome received lacrimal punctal plug insertion with the Punctal Plug F (FCI Ophthalmics) and 30 patients received plug insertion with the Super Flex plug (Eagle Vision; Softplug-Oasis Medical Inc). In total, 110 plug insertion regions were performed using the Punctal Plug F (group A) and 110 insertion regions were carried out using Super Flex plug (group B). The gauging system of Eagle Vision was used before the lacrimal punctal plug insertion in all subjects. Plug conditions (retention rates, spontaneous plug loss, and removal) and complications related to lacrimal punctal sizes were compared between the 2 groups.
Results
Retention rates were 70.4% in group A and 30.1% in group B at 6 months. Spontaneous plug loss occurrence was significant with the larger lacrimal punctum size in group A ( P < .05), whereas no significant differences were observed between lacrimal punctum sizes and spontaneous loss in group B. Spontaneous plug loss occurrence was significant in elderly patients in group B ( P < .05). Granuloma and injector troubles were observed in 1 and 2 cases in group A, respectively.
Conclusions
The Punctal Plug F seems to be more applicable for insertion into the smaller punctal sizes. Punctum size and age seem to be important factors in determining the appropriate types of lacrimal punctal plugs.
Silicone plug insertion has been recognized as a safe, effective, and reversible method to preserve aqueous and artificial tears on the ocular surface and is used widely for punctal occlusion to reduce the signs and symptoms of dry eye. Several complications of lacrimal punctal plugs, however, have been reported, such as corneal or conjunctival abrasion by the exposed portion of the plugs, acute conjunctivitis associated with biofilm formation on the lacrimal punctal plug, intracanalicular migration, formation of granuloma, canalicular stenosis, plug extrusion, and spontaneous plug loss.
Spontaneous plug loss is an important problematic issue associated with lacrimal punctal plug occlusion. Several studies have shown that the rate of spontaneous plug loss varies between 20% and 50%. Various materials and designs of the plugs are now available. The Super Flex punctal plug (Eagle Vision, Memphis, Tennessee, USA; Softplug-Oasis Medical Inc, Glendora, California, USA) has been used wildly in Japan because the plug can be inserted easily by general ophthalmologists. The FCI lacrimal punctal plug (FCI Ophthalmics, Issy-les-Moulineaux Cedex, France) has such advantages as a lower rate of spontaneous plug loss compared with the Super Flex plug. However, ophthalmologists may experience problems during the insertion procedure because of the structural features. Recently, a new model of the FCI plug has been introduced named the Punctal Plug F, of which the plug head pulled by the injector is sharp and is inserted easily using only perpendicular pressure. It also has been reported that punctal size is enlarged after extraction of lacrimal punctal plugs. However, few studies have described the retention rates and complications related to punctal sizes. In this study, we investigated the retention rates and complications related to Punctal Plug F insertion compared with Super Flex plug insertion with the focus on the relationship with punctum sizes.
Methods
The study followed the tenets of the Declaration of Helsinki. Informed consent for this research using 1 of the 2 different types of lacrimal punctal plugs was obtained from all patients who agreed to participate after explanation of the nature and possible consequences of the study. This prospective study received institutional review board approval from the Ishida Eye Clinic.
Subjects
Forty-four dry eye patients (10 men and 34 women; mean age, 64.4 ± 18.3 years; range, 21 to 91 years) receiving lacrimal punctal plug insertion with the Punctal Plug F at the Wada Eye Clinic were enrolled, and 30 patients (4 men and 26 women; mean age, 58.2 ± 13.7 years; range, 30 to 78 years) receiving lacrimal punctal plug insertion with the Super Flex plug served as controls. Indications for lacrimal punctal plug treatment included aqueous deficient and short tear film break-up time types of dry eye, epitheliopathy occurring after penetrating keratopathy, superior limbic keratoconjunctivitis, and recurrent corneal erosion. Patients with moderate to severe dry eye syndrome (Schirmer test without anesthesia ≤5 mm or tear film break-up time ≤5 seconds) who previously used nonpreserved artificial tear drops without improvement of ocular surface findings and dry eye symptoms were included in the study. Patients with dacryocystitis or canaliculitis and a history of lacrimal surgical treatment were excluded. This was a prospective, nonrandomized, interventional, comparative study of the differences in plug retention rates and complications between these 2 groups. Patients who received the Punctal Plug F underwent the same examinations and same follow-up procedures as the group who received the Super Flex plug. Patient inclusion and exclusion criteria were the same, and the number of lacrimal punctal plug insertions was matched during the recruitment of the group who received the Super Flex plug. In total, 110 plug insertion regions were inserted using the Punctal Plug F in the current study (group A). Likewise, 110 insertion regions were carried out using the Super Flex plug (group B; Table 1 ). The patients in both groups were followed up for at least 1 month. Spontaneous loss was defined as the absence of a plug noted on a follow-up visit. Plug removal was defined as having occurred when the surgeons removed a plug for symptoms of epiphora or local discomfort.
| Lacrimal Punctal Size (mm) | Total | |||||||
|---|---|---|---|---|---|---|---|---|
| 0.4 | 0.5 | 0.6 | 0.7 | 0.8 | 0.9 | 1.0 | ||
| Group A a | ||||||||
| Upper | 0 | 22 | 21 | 12 | 7 | 6 | 1 | 69 |
| Lower | 5 | 5 | 14 | 9 | 7 | 0 | 1 | 41 |
| Group B b | ||||||||
| Upper | 8 | 17 | 27 | 8 | 7 | 0 | 0 | 67 |
| Lower | 1 | 13 | 13 | 15 | 1 | 0 | 0 | 43 |
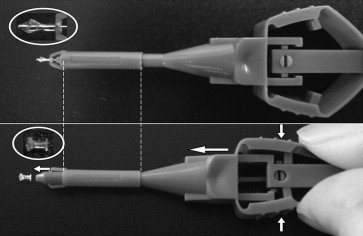
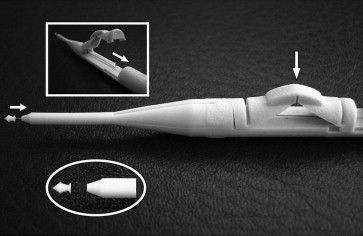
Lacrimal Punctal Plug Characteristics
Figure 1 shows the structural features of the Punctal Plug F. When released from the plug inserter, the plug resumes its natural expanded shape, which allows it to fit snugly in place and prevents plug pop-out. One size is available for all sizes of puncta. Figure 2 shows the structural features of the Super Flex plug. This device is available in 8 sizes from 0.4 to 1.1 mm on a 0.1-mm scale.
Lacrimal Punctal Plug Insertion
The gauging system of Eagle Vision was used before the lacrimal punctal plug insertion in all subjects. Plugs with a diameter 1 size larger than that measured by the gauge were inserted in group B in this study. Although the Punctal Plug F is regarded as being available for all lacrimal punctal sizes, we measured punctal sizes using the same gauging system in group A. Topical anesthesia was not applied before lacrimal punctal plug insertion to confirm that there was no local discomfort resulting from lacrimal punctal plugs.
The Punctal Plug F was inserted with the standard technique simply with gentle pressure, and the Super Flex plug was inserted with the technique described in our previous report by 2 experienced surgeons (M.K., R.I.).
We plugged both the lower and upper puncta in severe dry eye cases on the first insertion and only the upper puncta in the mild dry eye cases initially. The application of the plug insertion to the upper punctum in the mild cases is based on our previous report.
Statistical Analysis
Plug conditions (retention rates, spontaneous plug loss, and removal) related to lacrimal punctal sizes were compared between groups A and B using the chi-square test. Other complications (acute infection of the lacrimal drainage system, granuloma formation, and intracanalicular migration) related to lacrimal punctal size were analyzed. The relationship between age and spontaneous plug loss was analyzed by a paired t test. SPSS software version 12.0J for Windows (SPSS Inc, Chicago, Illinois, USA) was used as the statistical analysis software. A P value of less than .05 was considered statistically significant.
Results
Lacrimal Punctum Size and Insertion Region of the Lacrimal Punctal Plugs
Table 1 shows the details of lacrimal puncta sizes in groups A and B. No significant differences were observed in lacrimal puncta sizes between the 2 groups. The mean size of the lower and upper lacrimal punctae were 0.61 ± 0.12 mm and 0.60 ± 0.13 mm, and no significant differences were observed between the lower and upper lacrimal punctae ( P > .05).
Retention Rates of Lacrimal Punctal Plugs
Table 2 shows the details of the plug status of plug retention, spontaneous loss, and removal at 1, 3, and 6 months. Retention rates were 57 (70.4%) plugs in group A and 25 (30.1%) plugs in group B at 6 months. Three Punctal Plug Fs were removed because of symptoms of epiphora (1 plug) and partial plug extrusion (2 plugs). Five Super Flex plugs were removed by us within the 6 month follow-up period because of the symptoms of epiphora.
| Group | In Place (%) | Spontaneous Loss (%) | Removal (%) | Total (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Month | 3 Months | 6 Months | 1 Month | 3 Months | 6 Months | 1 Month | 3 Months | 6 Months | 1 Month | 3 Months | 6 Months | |
| A a | 104 (94.5) | 82 (85.4) | 57 (70.4) | 6 (5.5) | 11 (11.5) | 21 (25.9) | 0 (0) | 3 (3.1) | 3 (3.7) | 110 (100) | 96 (100) | 81 (100) |
| B b | 89 (80.9) | 46 (48.4) | 25 (30.1) | 20 (18.2) | 44 (46.3) | 53 (63.9) | 1 (0.9) | 5 (5.3) | 5 (6.0) | 110 (100) | 95 (100) | 83 (100) |
Spontaneous Loss of Lacrimal Punctal Plugs
Spontaneous plug loss was observed in 25.9% in group A and in 63.9% in group B at 6 months ( Table 2 ). Table 3 shows the details of spontaneous loss related to lacrimal punctum sizes at the 6-month follow-up. Spontaneous plug loss tended to occur significantly in the larger lacrimal punctum size in group A ( P < .05), whereas no significant differences were observed in the relationship between lacrimal punctum sizes and spontaneous loss in group B. No significant differences were observed in the rate of spontaneous loss between lower and upper puncta in both groups ( P > .05). The mean ages of the patients with the plug retention and spontaneous loss were 66.0 ± 16.6 years and 58.2 ± 22.3 years in group A and 53.1 ± 14.8 years and 62.8 ± 11.1 years in group B. With regard to the analysis of age and plug loss, the patients who lost plugs spontaneously were significantly older than the patients who maintained plugs in the puncta in group B ( P < .05), whereas no association was observed between age and plug loss in group A.



