Purpose
To compare choroidal thickness and extent and density of drusen between eyes with typical exudative age-related macular degeneration (AMD) and eyes with retinal angiomatous proliferation (RAP).
Design
Observational case series.
Methods
Twenty-four eyes with typical exudative AMD and 20 eyes with RAP were included. Subfoveal choroidal thickness was measured using enhanced depth imaging optical coherence tomography. Eyes were classified into 3 groups according to the extent of drusen distribution in the fundus photograph. Density of drusen was estimated based on optical coherence tomography images of the fellow eye. The proportion of the length beneath the drusen per the entire length of the Bruch membrane was defined as the density of drusen. Subfoveal choroidal thickness, extent of drusen distribution, and the density of drusen were compared between typical exudative AMD and RAP.
Results
Mean ± standard deviation subfoveal choroidal thickness in eyes with typical exudative AMD and eyes with RAP was 184.9 ± 68.5 μm and 139.0 ± 65.5 μm, respectively ( P = .035). The mean density of drusen was 0.06 ± 0.08 and 0.24 ± 0.12, respectively ( P < .001). In the typical exudative AMD group, 19, 3, and 2 eyes were included in the small extent group (<one third), intermediate extent group (one third to two thirds), and large extent group (>two thirds), respectively. In the RAP group, 3, 14, and 3 eyes were included in each aforementioned group, respectively ( P = .001).
Conclusions
The thinner subfoveal choroidal thickness and greater extent and density of drusen in RAP than the typical exudative AMD may suggest compromised choroidal perfusion in the development of RAP.
The functional and structural status of the choroid is associated closely with the development of age-related macular degeneration (AMD). Choriocapillaris dropout has been observed in areas adjacent to active choroidal neovascularization (CNV). Foveolar choroidal blood flow was reduced in eyes with AMD. In addition, the development of the CNV and visual loss are associated with lower choroidal blood volume and flow.
Retinal angiomatous proliferation (RAP) is a variant of exudative age-related macular degeneration (AMD) characterized by intraretinal neovascularization and retinal–retinal anastomosis, retinal–choroidal anastomosis, or both. There is controversy regarding whether the origin of RAP is the retina or the choroid. However, it is necessary to differentiate RAP from other forms of exudative AMD because of its poor prognosis and high risk of neovascularization in the fellow eye. Although some investigators have suggested that the outer retinal ischemia induced by reduced choroidal perfusion may be one possible reason, the exact mechanism underlying the development of this peculiar form of vasculature remains to be elucidated.
Recent studies attempting to investigate the choroid in macular disorders have disclosed that the choroidal thickness of eyes with exudative AMD was generally thinner than that of normal eyes. Drusen are frequently observed in eyes with RAP. Because the presence of drusen is known to be associated with decreased choriocapillaris density and decreased choroidal blood flow, it is a factor to consider when investigating the choroid in eyes with RAP.
Different characteristics in the structural profile of the drusen and choroid between eyes with RAP and eyes with typical exudative AMD remain to be elucidated. In this study, we compared the subfoveal choroidal thickness between eyes with RAP and eyes with typical exudative AMD. The extent and density of drusen additionally were compared between the 2 disease groups.
Methods
This observational case series was performed at a single center. The study was approved by the Institutional Review Board of the Samsung Medical Center, Republic of Korea (Samsung Medical Center Institutional Review Board no. 2011-12-014). The methodology adhered to the tenets of the Declaration of Helsinki. We conducted a review of medical records of patients who were diagnosed with exudative AMD between October 1, 2009, and November 1, 2011. To be included in this study, subjects were required to undergo a comprehensive ophthalmologic examination, including measurement of best-corrected Snellen visual acuity, 90-diopter (D) lens slit-lamp biomicroscopy, fundus fluorescein angiography, and indocyanine green angiography with a confocal laser scanning system (HRA-2; Heidelberg Engineering, Dossenheim, Germany). All patients also had undergone a spectral-domain optical coherence tomography (OCT) examination (Spectralis, Heidelberg Engineering GmbH, Heidelberg, Germany) for both eyes. The choroidal thickness as well as extent and density of drusen were analyzed.
A diagnosis of exudative AMD was based on a combination of fundus photographs, fluorescein angiography findings, and indocyanine green angiography results, with evidence of hyperfluorescence and late leakage associated with pigment epithelial detachment, serous retinal detachment, subretinal exudation, and hemorrhage in the macular region. All eyes compatible with polypoidal choroidal vasculopathy that exhibited a branching vascular network, terminating polypoidal lesion(s), or both on indocyanine green angiography were excluded. The exudative AMDs were classified either as RAP or typical exudative AMD. Cases that exhibited evidence of retinal–retinal or retinal–choroidal anastomosis on indocyanine green angiography were classified as RAP. The other cases were classified as typical exudative AMD. If a patient was involved with typical exudative AMD or RAP in both eyes, only the right eye was included in this study. If a patient had RAP in one eye and typical exudative AMD in the fellow eye, only the eye with RAP was included. That is, only 1 eye was included from each subject.
The exclusion criteria included the presence of refractive errors of more than ±3.0 D; amblyopia; significant media opacity or thick subfoveal hemorrhage; evidence of end-stage AMD such as central geographic atrophy or disciform scar; findings of ocular inflammation, retinal detachment, photodynamic therapy, vitrectomy, any other intraocular surgery (including cataract surgery) in the study eye within 1 year, ocular trauma, or glaucoma in the study eye. Eyes with a history of intravitreal triamcinolone injection also were excluded; however, eyes that had undergone anti–vascular endothelial growth factor (VEGF) treatment more than 3 months previously were included.
Subfoveal Choroidal Thickness
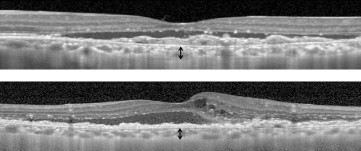
Enhanced depth imaging OCT was conducted based on previously described methods. By using the Heidelberg Eye Explorer software version 1.5.12.0, the choroidal thickness was measured manually as previously described. Choroidal thickness was defined as the vertical distance from the hyperreflective line of the Bruch membrane to the innermost hyperreflective line of the chorioscleral interface ( Figure 1 ). Because we experienced a discrepancy in the choroidal thickness measurements between measurements based on 1:1-pixel image and those based on 1:1-μm image in certain cases, all the measurements were performed based on the latter. The subfoveal choroidal thickness was compared between the eyes with RAP and typical exudative AMD. Intragroup comparison of differences in subfoveal choroidal thickness between the first and the last visits was conducted for both the RAP group and the exudative AMD group. The subfoveal choroidal thickness of fellow eyes without exudative change also was compared between the 2 disease groups.
Extent and Density of Drusen
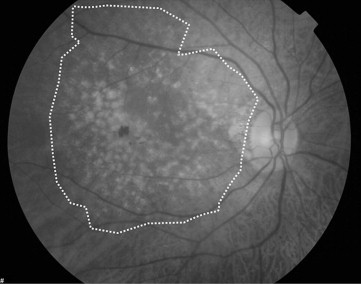
Fundus photographs of the posterior retina (30 degrees in diameter centered at the foveal center) were obtained. The extent of distribution of intermediate drusen (63 to 124 μm in diameter) and soft drusen (≥125 μm in diameter) was estimated based on fundus photographs. Studied eyes were classified into 3 groups according to their extent of distribution of drusen in the fundus photographs: small extent group, less than one third of the extent of the fundus photograph; intermediate extent group, one third to two thirds of extent of the fundus photograph; and large extent group, more than two thirds of extent of the fundus photograph ( Figure 2 ). If no drusen were observed, the eye was classified as being in the small extent group. The extent of distribution of drusen was compared between the RAP group and the typical exudative AMD group.
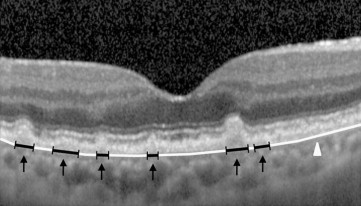
The density of drusen in the fellow eye was determined by the horizontal and vertical crosshair enhanced depth imaging OCT scans through the fovea. Because the density of drusen could not be determined accurately in eyes with exudative change, only images of fellow eyes without exudative change were assessed. All images on OCT were converted to gray scale for better visualization and then were imported to Image J (freeware; National Institute of Health, Bethesda, Maryland, USA) for analysis. The entire length of the Bruch membrane within 3000 μm in diameter centered at the foveal center was measured using a segmented line tool. The total length of the Bruch membrane beneath the drusen, located within 3000 μm in diameter centered at the foveal center, also was measured using a segmented line tool ( Figure 3 ). In our pilot study, it was difficult to measure accurately the diameters of drusen that were smaller than 70 μm. Thus, we defined diameters of 70 μm or more as a measurable size, and the measurements were obtained only for measurable sizes of drusen. The density of drusen was calculated as the total length of the Bruch membrane beneath the drusen divided by entire length of the Bruch membrane, and the mean density of drusen obtained from both horizontal and vertical scans was used for analysis. The density of drusen was compared between the RAP group and the typical exudative AMD group. Correlation between the density of drusen and subfoveal choroidal thickness was estimated in the fellow eyes of patients with both RAP and typical exudative AMD. In addition, the diagnostic value of the extent of drusen and choroidal thickness for diagnosing RAP was analyzed.
All the measurements were conducted by a single trained examiner (J.H.K.). Statistical analyses were performed with a commercially available software package (SPSS version 18.0 for Windows; SPSS Inc, Chicago, Illinois, USA). A test of normality was performed using the Shapiro-Wilk test. Values of baseline characteristics were compared using the Mann–Whitney U test and chi-square test. Comparison of subfoveal choroidal thickness between the 2 disease groups was performed using the Mann–Whitney U test. The subfoveal choroidal thickness and density of drusen of the fellow eyes were compared using the Mann–Whitney U test. The correlation between the density of drusen and subfoveal choroidal thickness in fellow eyes was estimated using the Spearman correlation analysis. Comparison of the subfoveal choroidal thickness between 2 time points was performed using the Wilcoxon signed-rank test. A comparison of the distribution of eyes among groups for the extent of drusen was performed using the Cochran-Armitage test. In addition, the diagnostic value and cutoff value of the extent of drusen and choroidal thickness were estimated using univariate logistic regression with receiver operating characteristic curve analysis. A P value less than .05 was considered significant.
Results
Twenty-four eyes of 24 patients with typical exudative AMD and 20 eyes of 20 patients with RAP were included in this study. The difference in age (74.0 ± 7.4 years vs 76.8 ± 7.3 years; P = .357), spherical equivalent (0.78 ± 0.91 D vs 0.56 ± 0.63 D; P = .115), and sex distribution (male to female, 10:14 vs 6:14; P = .534) were not significant between the typical exudative AMD group and the RAP group. In the RAP group, 4 (20%), 9 (45%), and 7 (35%) eyes were verified to have stage 1, 2, and 3 RAP lesions, respectively, in accordance with the classification established by Yannuzzi and associates. The mean duration of symptoms was 3.79 ± 3.31 months (range, 1 to 12 months) in 19 eyes with RAP. The time of onset of visual symptoms could not be estimated accurately in 1 eye with best-corrected visual acuity of 20/50.
Four eyes with typical exudative AMD and 1 eye with RAP had undergone cataract surgery more than 1 year previously. In these eyes, spherical equivalents before cataract surgery were used for analysis. Two eyes with RAP received intravitreal anti-VEGF injections 3 months before they underwent the first enhanced depth imaging OCT scan and the other eyes in both disease groups were naïve to treatment.
The Table summarizes the difference in subfoveal choroidal thickness, extent of drusen, and density of drusen between the 2 disease groups. The mean subfoveal choroidal thickness on the initial manifestation in eyes with typical exudative AMD and eyes with RAP was 184.9 ± 68.5 μm (range, 94.0 to 294.5 μm) and 139.0 ± 65.5 μm (range, 66.0 to 371.0 μm), respectively ( Figure 4 ). The choroid was significantly thinner in the eyes with RAP than the eyes with typical exudative AMD (0=.035). Patients with typical exudative AMD had a mean follow-up of 8.9 ± 5.9 months after the first enhanced depth imaging OCT examination.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


