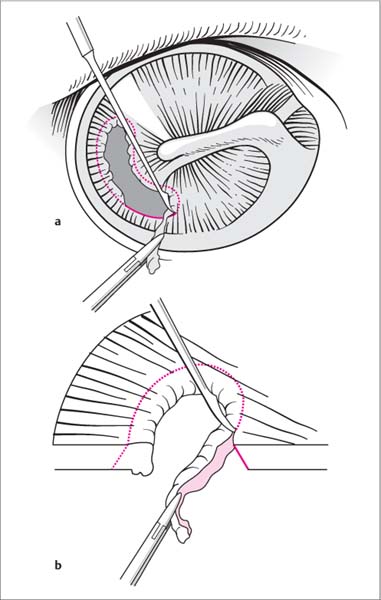
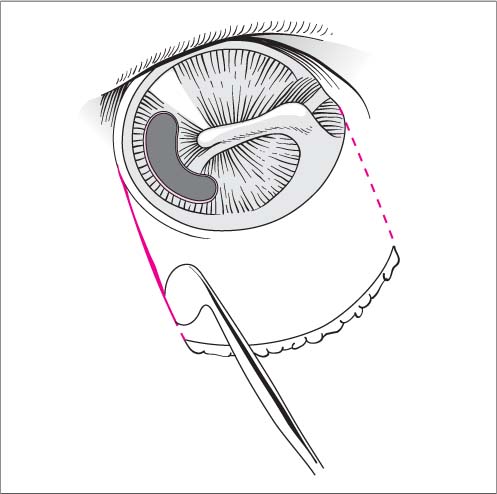
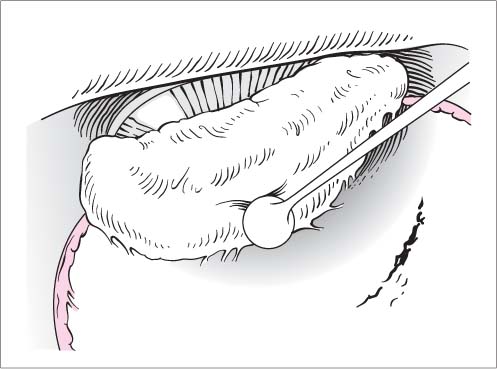
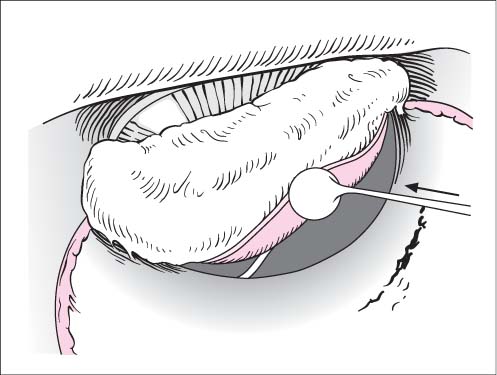
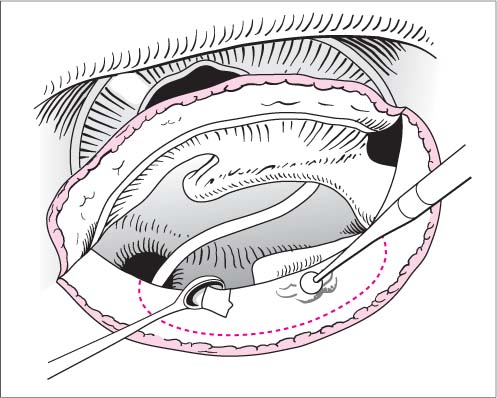
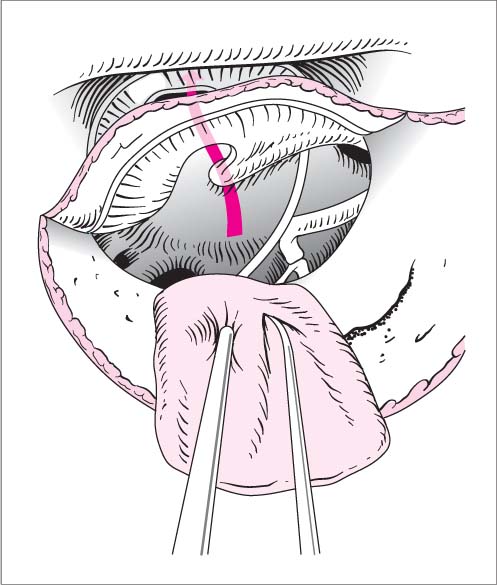
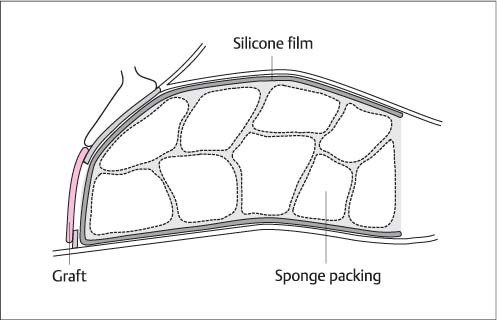
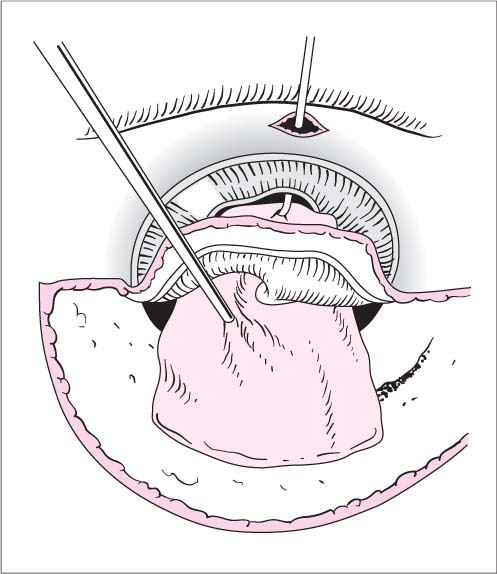
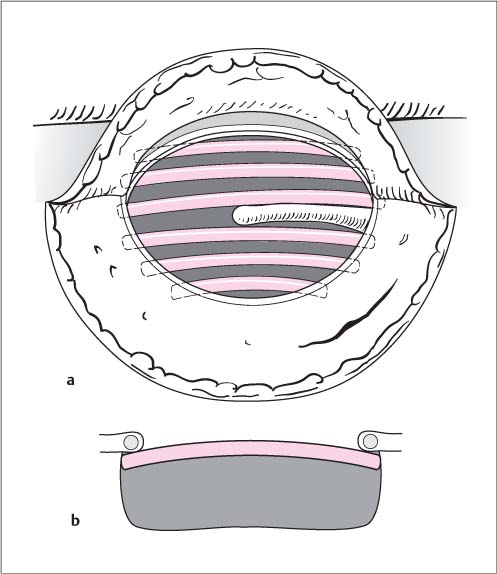
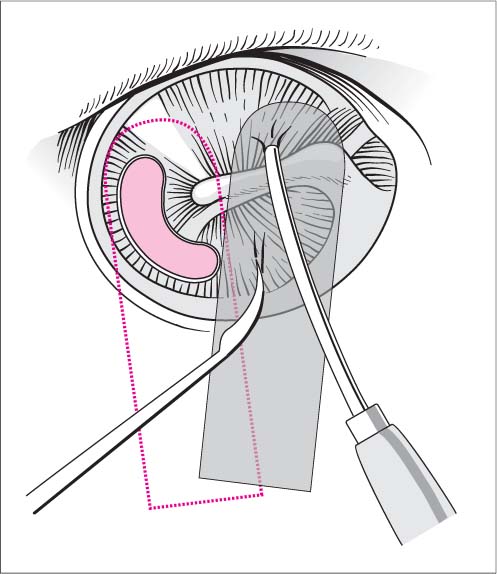
18 Tympanoplasty Local or general anesthesia. Positioning. The patient is positioned supine with the head turned to the side and immobilized on a headrest or ring. Approach. Endaural or postauricular (Chapter 17). The graft is harvested, and the plane of the tympanic membrane is adequately exposed with self-retaining retractors. If necessary, the entrance to the ear canal can be enlarged with a burr. Recipient bed. The margins of the perforation are freshened by cutting around them with a sickle knife held at an oblique angle to the tympanic membrane. A microforceps grips the resected tissue with the margins under tension (Fig. 18.1a, b). This step is always completed before the tympanic annulus is separated from the sulcus. Tympanomeatal flap. The tympanomeatal flap is outlined with a straight round knife. Cuts are made at the 11 and 5 o’clock positions in the right ear and at 1 and 7 o’clock in the left ear (see Fig 17.3 and Fig. 18.2; see also Chapter 17). The meatal flap is elevated toward the tympanic membrane from the bone with an angled round incision knife, aided by a suction tip (Fig. 18.3). Fig. 18.1a, b Tympanoplasty. a The margins of the tympanic membrane perforation are freshened with a sickle knife while a microforceps keeps the margins tense. b The knife is angled relative to the plane of the tympanic membrane. Fig. 18.2 Tympanoplasty. Outlining the tympanomeatal flap. Fig. 18.3 Tympanoplasty. The tympanomeatal flap is elevated from the bone. Opening the middle ear cavity. The middle ear cavity is opened in the posterosuperior quadrant, where the annulus is easier to detach from the sulcus. As the tympanomeatal flap is raised, the thin mucoperiosteum becomes tense and can be divided without damaging the chorda tympani. The annulus fibrosus is dissected from the sulcus below the attachment of the chorda tympani, using first a sickle knife and then a round incision knife. The mobilized tympanomeatal flap is reflected forward (Fig. 18.4). Evaluation of the ossicular chain. The bony posterolateral attic wall (area that can be under-run with a round knife) is taken down with the House curette—after first thinning it with a diamond burr if necessary—until the long process of the incus, the stapes, and the tympanic facial nerve segment can be identified (Fig. 18.5). At this point the manubrium of the malleus is probed very gently with a needle to assess the continuity and mobility of the ossicular chain. Graft selection. The graft (fascia, perichondrium, or cartilage) is sized so that it will safely overlap the perforation on all sides and extend slightly onto the posterior canal wall (to allow for shrinkage; see Chapter 17). Graft placement. The graft is introduced into the middle ear cavity with a needle and suction tip, allowing approximately 3 mm of overlap between the graft and perforation margins. The graft may be placed medial to the manubrium and is held in place by adhesion (underlay technique, Fig. 18.6). Later the posterior portion of the graft will be below the tympanomeatal flap and will slightly overlap the bony posterior wall of the ear canal. Fig. 18.4 Tympanoplasty. The middle ear cavity is opened in the posterosuperior quadrant. The mucoperiosteum is divided while the chorda tympani is preserved. Fig. 18.5 Tympanoplasty. The posterolateral attic wall is taken down so that the ossicular chain can be assessed. Fig. 18.6 Tympanoplasty. The graft is placed behind the tympanic membrane and medial to the manubrium (underlay technique). Returning the flap. The tympanomeatal flap is returned to its original position with meticulous reapproximation of the flap margins. Rounded silastic strips (Fig. 18.7) are placed into the ear canal to cover the junction of the replaced meatoplasty and tympanomeatal flap while also supporting the graft from the lateral side (Fig. 18.8). Wound closure. The ear canal is packed with antibiotic-impregnated gelatin sponge and short, superficial strips. The wound is closed in layers. Modified underlay technique. With a lack of residual anterior membrane, the graft can be delivered to the repair site using a pull-through technique. The anterior annulus is undermined to the bone at one or two points with a sickle knife, and one end of the graft is pulled through the tunnel to the plane of the tym-panic membrane with a tiny hook or suction tip (Fig. 18.9). If an adequate margin is present, the same technique can be used on the anterior pars tensa without undermining the annulus. Onlay technique. The epithelium is elevated from the tym-panic membrane surface along with the manubrium and returned after the graft has been placed on the tunica propria. The margins of the perforation are freshened, and the tympanomeatal flap is dissected with an angled round knife over the firmly adherent posteroinferior annulus onto the tunica propria. In this way the tympanic membrane epidermis can be developed anteriorly in continuity with the tympanomeatal flap. It is dissected from the manubrium and short process with a sickle knife. There is a risk that a flap cholesteatoma may form as a result of residual squamous epithelium, and blunting of the tympanomeatal angle may occur. Advantages are a more stable anterior graft placement and a normal volume of the middle ear cavity. Myringoplasty. Special type of type I tympanoplasty: The tympanic membrane is closed with an underlay technique without evaluating the ossicular chain and without mobilizing the posterior annulus (prerequisites are a healthy tympanic membrane and middle ear and no conductive impairment). Generally this procedure involves an endaural approach with an autologous graft, freshening the perforation with a sickle knife, and removing the rim of loose epithelium with a cup forceps. A small fascial graft is introduced through the perforation and approximated to the medial surface of the tympanic membrane with a needle and suction tip. Reperforations. Small reperforations: With a dry middle ear, the margins of the perforation are freshened with a sickle knife and the epithelial rim is removed. A pressed, postauricular fat-connective tissue graft is passed through the perforation with a needle, approximated with a microsuction tip, and covered laterally with silastic film. Larger reperforations require a repeat tympanoplasty, which is done after sequelae and swelling from the initial procedure have subsided. Perichondrium. This material is best suited for small to medium-sized tympanic membrane defects that are susceptible to infection. It is similar to fascia in its workability and handling. Cartilage. Cartilage is preferred for reconstructing subtotal defects, closing defects associated with poor ventilation or retraction pockets, recurrent perforations, and infection-prone ears. The palisade technique is particularly useful for very anterior defects without adequate margins, impaired eustachian tube ventilation, and adhesive processes. Cartilage–perichondrium composite grafts with a cartilage disk are excellent for reconstructing subtotal defects or old welding spatter injuries. The central cartilage disk (see Chapter 17, p. 365) is placed with its perichondrial side against the tym-panic membrane. It can also be incised for easier application, or a portion may be excised to accommodate the (de-epithelial ized) manubrium (“under-overlay” technique). A pure cartilage disk graft is worked and used in much the same way. Fig. 18.7 Tympanoplasty. Inserting the silastic film. Fig. 18.8 Tympanoplasty. Longitudinal section of the ear canal shows the graft position, gelatin sponge packing, and silastic film. Palisades. Approximately six precut cartilage struts (see Chapter 17, p. 365) are wedged into place beneath the tym-panic membrane from one side of the perforation to the other, all directed parallel to the manubrium. They are shortened according to their position so that their intrinsic tension creates a slight bow (Fig. 18.10a, b). The struts are covered laterally with perichondrium or fascia. Fig. 18.9 Tympanoplasty. Modified underlay technique for a deficient anterior recipient bed. The graft is grasped at one end and pulled into place. Fig. 18.10a, b Tympanoplasty. Palisade technique. a The palisades are placed parallel to the manubrium. b They are wedged into a slightly bowed position within the middle ear cavity. An ossicular chain reconstruction follows evaluation of the ossicular chain and the eradication of middle ear disease. It is done after the tympanic membrane graft has been placed and before the tympanomeatal flap is replaced to close the middle ear cavity. The reconstructive measures vary according to the location and extent of the ossicular defect. A defect in the lenticular process or incudostapedial joint is reconstructed and bridged with glass ionomer cement. While still malleable, a small bead of cement is placed on the head (capitulum) of the stapes and shaped with a round knife or Rosen elevator to form a connection with the incus. This process can be repeated if necessary during the several minutes it takes for the cement to harden. Before the cement is applied, the oval and round windows should be protected from accidental contact (e. g., covered with Gelfoam). Conversion to a type IIIA tympanoplasty by interposition (see below). The defect is bridged with a partial ossicular chain replacement prosthesis (PORP) (stapes elevation) consisting of autologous ossicles or synthetic material (preferably a titanium implant, see Chapter 17).
Surgical Principle
 Tympanoplasty encompasses a range of surgical measures to improve hearing and eradicate disease in patients with chronic otitis media, tympanic membrane perforation, or ossicular discontinuity.
Tympanoplasty encompasses a range of surgical measures to improve hearing and eradicate disease in patients with chronic otitis media, tympanic membrane perforation, or ossicular discontinuity.
 The tympanic membrane can be reconstructed with fascia, perichondrium, or cartilage. The ossicular chain can be reconstructed with autologous or synthetic material. This chapter reviews the basic techniques involved in reconstructing the tympanic membrane and ossicular chain and eradicating disease in the middle ear cavity or mastoid.
The tympanic membrane can be reconstructed with fascia, perichondrium, or cartilage. The ossicular chain can be reconstructed with autologous or synthetic material. This chapter reviews the basic techniques involved in reconstructing the tympanic membrane and ossicular chain and eradicating disease in the middle ear cavity or mastoid.
 The classic Wullstein classification of tympanoplasties is expanded by adding two subgroups to the type III reconstruction: A, in which the stapes is present, and B, in which only the footplate is present.
The classic Wullstein classification of tympanoplasties is expanded by adding two subgroups to the type III reconstruction: A, in which the stapes is present, and B, in which only the footplate is present.
Indications
 Dry or wet, central or peripheral tympanic membrane perforation with or without an ossicular discontinuity, possibly after prior surgery for inflammatory middle ear disease.
Dry or wet, central or peripheral tympanic membrane perforation with or without an ossicular discontinuity, possibly after prior surgery for inflammatory middle ear disease.
 Adhesive processes, tympanosclerosis, sequelae to a petrous bone fracture or middle ear trauma, suspected ossicular discontinuity following an old antrotomy.
Adhesive processes, tympanosclerosis, sequelae to a petrous bone fracture or middle ear trauma, suspected ossicular discontinuity following an old antrotomy.
 Candidates for an ossicular reconstruction should have an air-bone gap of at least 20 dB and acceptable inner ear function.
Candidates for an ossicular reconstruction should have an air-bone gap of at least 20 dB and acceptable inner ear function.
Contraindications
 Deafness in the opposite ear (relative).
Deafness in the opposite ear (relative).
 Limited capacity for follow-up care, as in small children (relative).
Limited capacity for follow-up care, as in small children (relative).
 Poor inner ear function (drainage only).
Poor inner ear function (drainage only).
 Otogenic complications (relative, may necessitate a two-stage procedure).
Otogenic complications (relative, may necessitate a two-stage procedure).
 Simultaneous tympanoplasty in both ears (a 3-month interval should elapse between the two procedures).
Simultaneous tympanoplasty in both ears (a 3-month interval should elapse between the two procedures).
 Very severe otorrhea and otitis externa (relative).
Very severe otorrhea and otitis externa (relative).
Specific Points Regarding Informed Consent
 Lack of hearing improvement, exacerbation of hearing loss, or deafness (may be delayed due to implant problems).
Lack of hearing improvement, exacerbation of hearing loss, or deafness (may be delayed due to implant problems).
 Tinnitus.
Tinnitus.
 Vertigo.
Vertigo.
 Altered taste sensation (chorda tympani).
Altered taste sensation (chorda tympani).
 Recurrent perforation, graft rejection, otorrhea, cholesteatoma formation, reoperation, second-look procedure.
Recurrent perforation, graft rejection, otorrhea, cholesteatoma formation, reoperation, second-look procedure.
 Intracranial complications.
Intracranial complications.
 Heavy scarring of the incision and auricle, keloid formation.
Heavy scarring of the incision and auricle, keloid formation.
 Neuralgiform pain.
Neuralgiform pain.
 Facial nerve injury.
Facial nerve injury.
 Patients may be told to avoid diving or flying for a certain period.
Patients may be told to avoid diving or flying for a certain period.
Surgical Principle
 PT, PTT, platelet count, simple blood count.
PT, PTT, platelet count, simple blood count.
 Complete audiometry, test for spontaneous nystagmus and fistula symptoms, Schüller radiograph, high-resolution CT if required.
Complete audiometry, test for spontaneous nystagmus and fistula symptoms, Schüller radiograph, high-resolution CT if required.
 Perioperative antibiotics may be indicated.
Perioperative antibiotics may be indicated.
Special Instruments
 Otomicroscope
Otomicroscope
 Small drill, variable speed to 40 000 rpm, with an angled handpiece; drill bits and burrs of varying size, shape (round, cylindrical, pear-shaped), and finish (diamond, hard metal).
Small drill, variable speed to 40 000 rpm, with an angled handpiece; drill bits and burrs of varying size, shape (round, cylindrical, pear-shaped), and finish (diamond, hard metal).
 Set of round incision knifes, small hooks, needles, curettes (House), antrum hooks, Rosen elevator.
Set of round incision knifes, small hooks, needles, curettes (House), antrum hooks, Rosen elevator.
 Assorted otologic microforceps (e. g., Heermann), cup microforceps, malleus head punch, middle ear scissors, Weingartner grasping forceps.
Assorted otologic microforceps (e. g., Heermann), cup microforceps, malleus head punch, middle ear scissors, Weingartner grasping forceps.
 Suction tips, microsuction tips, suction-irrigators.
Suction tips, microsuction tips, suction-irrigators.
 Bipolar coagulation.
Bipolar coagulation.
 Manual and self-retaining retractors (Plester, Helms).
Manual and self-retaining retractors (Plester, Helms).
Anesthesia
Reconstruction of the Tympanic Membrane
Type I Tympanoplasty
Surgical Technique
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 Graft overlap of the perforation margins should be sufficient to allow for graft shrinkage, and adequate contact should be established between the graft and manubrium.
Graft overlap of the perforation margins should be sufficient to allow for graft shrinkage, and adequate contact should be established between the graft and manubrium.
 Avoid lateralization of the tympanic membrane.
Avoid lateralization of the tympanic membrane.
 Placing gelatin sponge in the middle ear to support the graft should be done very sparingly, if at all, because of the risk of scar adhesions.
Placing gelatin sponge in the middle ear to support the graft should be done very sparingly, if at all, because of the risk of scar adhesions.
 The postauricular approach is better for very anterior perforations. A somewhat larger tympanomeatal flap is raised, extending to ca. 2 o’clock in the right ear and 10 o’clock in the left ear, to facilitate anterior pull-through of the graft.
The postauricular approach is better for very anterior perforations. A somewhat larger tympanomeatal flap is raised, extending to ca. 2 o’clock in the right ear and 10 o’clock in the left ear, to facilitate anterior pull-through of the graft.
 Scar adhesions or mucosal folds that obstruct ventilation should be divided.
Scar adhesions or mucosal folds that obstruct ventilation should be divided.
 Broad adhesions with the promontory wall or ossicular chain should be widely cleared while preserving the mucoperiosteum. The cartilage palisade technique is used for tympanic membrane reconstruction.
Broad adhesions with the promontory wall or ossicular chain should be widely cleared while preserving the mucoperiosteum. The cartilage palisade technique is used for tympanic membrane reconstruction.
 Nitrous oxide administration should be discontinued during graft placement as it may cause the graft to separate from the perforation.
Nitrous oxide administration should be discontinued during graft placement as it may cause the graft to separate from the perforation.
 Risks and Complications
Risks and Complications
 Iatrogenic cholesteatoma (flap cholesteatoma caused, for example, by incomplete detachment of the annulus from the sulcus).
Iatrogenic cholesteatoma (flap cholesteatoma caused, for example, by incomplete detachment of the annulus from the sulcus).
 Auricular perichondritis, distortion due to scarring.
Auricular perichondritis, distortion due to scarring.
 Conductive hearing loss due to ossicular dislocation or poor vibration characteristics of the graft.
Conductive hearing loss due to ossicular dislocation or poor vibration characteristics of the graft.
 Facial paralysis may be harmless and transient due to local anesthesia. Otherwise, immediate facial nerve reconstruction is required.
Facial paralysis may be harmless and transient due to local anesthesia. Otherwise, immediate facial nerve reconstruction is required.
 Sensorineural hearing loss, tinnitus, vestibular nerve damage (e. g., due to manipulation of the ossicular chain, contact with drill, suction or drilling noise).
Sensorineural hearing loss, tinnitus, vestibular nerve damage (e. g., due to manipulation of the ossicular chain, contact with drill, suction or drilling noise).
 Recurrent perforation, otorrhea, graft rejection.
Recurrent perforation, otorrhea, graft rejection.
 Altered taste sensation due to chorda tympani lesion.
Altered taste sensation due to chorda tympani lesion.
 Excessive scarring, keloid formation, neuralgiform pain.
Excessive scarring, keloid formation, neuralgiform pain.
 Meatal stenosis, epithelial defects.
Meatal stenosis, epithelial defects.
 Wound infection.
Wound infection.
Postoperative Care
 Perioperative antibiotics.
Perioperative antibiotics.
 Patients with postoperative infection or poor wound healing should receive broad-spectrum antibiotics until culture results are known.
Patients with postoperative infection or poor wound healing should receive broad-spectrum antibiotics until culture results are known.
 Packing is left in place for 3 weeks.
Packing is left in place for 3 weeks.
 Valsalva maneuvers are started on the first postoperative day.
Valsalva maneuvers are started on the first postoperative day.
 See Chapter 14 for details.
See Chapter 14 for details.
Alternatives
Closure Technique
Graft Materials
Ossicular Chain Reconstruction
Lenticular Process Defect (Type II Tympanoplasty)
Surgical Technique
Alternative
Incus Defect or Loss (Type IIIA Tympanoplasty)
Surgical Principle
Incus-to-Stapes or Malleus-to-Stapes Reconstruction
Indications
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


