11 Surgery of the Neck The nature of the surgical procedure determines the risk of postoperative wound infection. A general distinction is made between aseptic and septic wounds. Examples of aseptic procedures are the excision of a simple neck cyst or lymph node. The term “clean-contaminated wounds” is used when an incision is made in the neck and connects with the salivary system. Septic wounds include traumatically or preoperatively infected wounds as well as surgically inflicted wounds in which the pharyngeal mucosa has been opened at operation. The organisms most commonly identified in the neck are Staphy lococcus aureus and S. epidermidis, α-hemolytic streptococci, and especially Gram-negative organisms such as Klebsiella species, Proteus mirabilis, Pseudomonas aeroginosa, Escherichia coli, enterococci, and Enterobacter species. Second-generation cephalosporins have proven useful in the prevention of infection, but because their efficacy against some members of the Enter-obacteriaceae family (Klebsiella, Proteus, E. coli) is not complete, a cephalosporin should be combined with metronidazole in any operation that opens the pharynx. The standard practice in noninflammatory surgery is to administer a single dose of perioperative antibiotic. A cephalosporin and/or metronidazole should be administered intravenously 30–60 minutes before the start of the operation to achieve active serum and tissue levels. An adequate level of efficacy is maintained for approximately 3 hours, and longer operations will require an additional dose. In procedures that open the pharynx, the large wound surfaces require a 3- to 5-day course of second-generation cephalosporin plus metronidazole. Fever, leukocytosis, an elevated C-reactive protein (CRP), and/or cervical redness in the wound area may be the earliest signs of a postoperative wound infection. In patients with a frank postoperative wound infection, a specimen should be taken from the infected site for microbial analysis. Specific antibiotic therapy can then be administered on the basis of sensitivity results. Purulent soft-tissue infections should be evacuated and, if necessary, irrigated with an antiseptic solution (e. g., povidone iodine, Betaisodona) several times daily for several days. A postoperative infection in the neck is occasionally associated with a defect in the cervical soft tissues as a result of thrombophlebitis. If the infection persists, this may lead to the formation of extensive pharyngocutaneous fistulas. With proper treatment, however, the wound will usually undergo secondary healing by granulation. Inflammatory swellings in the neck are managed by a staged therapeutic approach. In the absence of liquefaction, cellulitis, sepsis and laryngeal edema, treatment is conservative and consists of antibiotic therapy. It may also be necessary to locate and eradicate an inflammatory focus in the tonsils, tongue, oral floor, teeth, or salivary glands. An abscess, on the other hand, requires immediate surgical drainage. The abscess is opened and drained with respect for skin cleavage lines while preserving nerves and vessels that cross the operative field. The indications are abscess formation and liquefaction (e. g., nonspecific inflammations, specific inflammations, actinomycosis, secondary inflammation of neck cysts). There are almost no contraindications, because of the risk of sepsis. The pathogenesis of the abscess should be investigated at the time of diagnosis. Possibilities includes inflammatory skin diseases and diseases of the Waldeyer ring. Dentogenic abscesses are also common. Dressing forceps, drainage material (e. g., Easy-Flow-Drainage). General or local anesthesia (Dermajet may be used for intracutaneous injection). One has to wait longer for local anesthesia to take effect in infected case due to change of pH in the tissues. Incision. The abscess is drained through a skin incision placed along RSTL over the mass. Generally the incision is 1–2-cm long. Introducing the dressing forceps and opening the abscess. The dressing forceps is introduced through the incision, parallel to the course of the major neck vessels. Guided by external palpation, the abscess is located with the forceps, spread open, and drained. Entry into the abscess is usually indicated by the immediate drainage of purulent material (a sample is taken for analysis). Draining the abscess. The dressing forceps is brought out below the abscess through an incision made over the forceps tip and opened wide enough to grasp the end of a drain (e. g., Easy-Flow-Drainage) and pull it upward through the abscess cavity. Securing the drain. The drain sutured to the skin above and below with simple interrupted sutures. Irrigation. At the end of the procedure, the drain is used to irrigate the abscess cavity with an antiseptic solution (e. g., povidone iodine, 11 % Betaisodona solution). A sample is taken so that specific antibiotics can be administered at operation. Because the organisms identified in an abscess smear will generally include anaerobes, a combination of agents (e. g., a cephalosporin plus metronidazole) should be used for initial therapy. Additionally, tissue should be taken from the abscess membrane for histological or molecular diagnostic analysis to check for an underlying classic or atypical tuberculosis. Sterilized safety pins can also be used to secure the drain. Easy-Flow-Drainage. Before insertion, elliptical openings ca. 1 cm long are cut in the lateral edges of the drain to allow for drainage of the antiseptic irrigating solution during the next few days. Septic complications; cellulitis; injuries to the marginal mandibular branch of the facial nerve, accessory nerve, recurrent laryngeal nerve, jugular vein, or other major vessels; postoperative bleeding; mediastinitis; laryngeal edema; keloid formation. Antibiotic therapy. The abscess may have to be reopened and drained. The drain is shortened and may be removed as the drainage volume declines. The wound heals secondarily, and scar revision may be elected at a later date. If an underlying cyst is present, it should be extirpated after inflammation has resolved. A 6-month course of penicillin is indicated for patients with actinomycosis. Removal of one lymph node or several conglomerated lymph nodes for histological examination. Persistent, noninflammatory lymph node swelling that requires benign–malignant differentiation. B-mode ultrasonography. Fine-needle aspiration cytology may be necessary in some cases. Sectional imaging modalities (CT, MRI) are rarely necessary. General endotracheal anesthesia, which may be supplemented by local anesthesia with a vasoconstrictor to reduce bleeding. Local anesthesia alone is an option in some patients. Skin incision. The skin incision of choice depends on the location of the lymph node and should follow the RSTL (Fig. 11.1). Dissection of subcutaneous fat. After division of the skin, the subcutaneous fat is spread open and secured with a retractor. The tissue planes are successively spread open to enter the lymph node-bearing compartments. Dissection at level I (submental and submandibular nodes). Particular attention is given to the marginal mandibular branch of the facial nerve in dissections of the submandibular nodes. The external incision is deepened through the platysma, and the posterior part of the wound is spread open to expose the facial vein, which is ligated and reflected upward. Localization of the lymph nodes is aided by manual or bimanual palpation while the oral floor is pushed forward (after first rinsing the oral cavity with antiseptic solution). Dissection at levels II–IV. Excisional biopsies are taken in proximity to the vascular sheath. Identification of the vascular sheath may be aided by locating the point where the omohyoid muscle crosses over the sheath. Dissection at level V. The accessory nerve occupies a very superficial location in the posterolateral triangle of the neck. Blunt dissection always proceeds parallel to the nerve, alternately pushing the connective tissue and fat aside with a dissecting sponge. Small vessels are coagulated with bipolar cautery. The accessory nerve is carefully identified. Exposing and freeing the lymph nodes. The lymph nodes are freed by blunt retraction and incision of the surrounding connective tissue bands. The lymph nodes themselves should not be grasped with a forceps or clamp, as this would hamper histological evaluation. Surrounding structures are held aside with retractors while the node is shelled out, aided if necessary by packing a gauze strip beneath it (the end should be left protruding). Hemostasis. Hemostasis must be meticulous. A large wound cavity should be closed in layers over a small suction drain. Fig. 11.1 Cervical lymphadenectomy. External incisions along the RSTLs. Note the nerve locations: the marginal mandibular branch of the facial nerve (1) in the submandibular region (the facial artery and vein are ligated and reflected upward) and the accessory nerve (2) behind the sternocleidomastoid muscle. If a large venous vessel is opened but cannot be grasped directly, it should be immediately packed off to prevent air embolism (unless endotracheal anesthesia is being used). Management of Injury to Large Arterial Vessels Arterial bleeding that cannot be immediately controlled should be packed off and the incision extended. Surrounding anatomical structures are identified, and the vessel is located and secured proximal to the site of the injury. The vessel is compressed proximal to the bleeding site with a mounted sponge. With injury to the common or internal carotid artery, consultation with a vascular surgeon may be necessary. Otherwise the head and neck surgeon may apply gentle, local compression with a small sponge, moving the compression site progressively closer to the tear. Pressure is applied caudal to the exposed vascular segment, and the tear in the vessel wall is repaired with sutures (e. g., 5–0 Prolene; note the compression time). Management of Significant Nerve Injury With an accessory nerve lesion, identify the stumps. If a primary nerve repair cannot be done, the nerve ends should be tagged for a secondary repair, but this is rarely necessary. – the accessory nerve in the lateral cervical triangle – the marginal mandibular branch of the facial nerve in the submandibular region; the lingual nerve may also be at risk in very deep lymphadenectomies – in the vascular compartment: the vagus nerve, recurrent laryngeal nerve, hypoglossal nerve, carotid artery, and jugular vein (caution: air embolism) – at the supraclavicular level: the pleura, subclavian artery and vein, brachial plexus, and thoracic duct. Drains are removed when the drainage volume falls to 30 mL or less. Sutures are removed on day 7. The entire prescalene fat pad is removed along with the palpable and nonpalpable lymph nodes that it contains. Severe debilitation. General endotracheal anesthesia is usually preferred. Local anesthesia is induced by infiltrating the area around the operative site. Caution: air embolism. Skin incision and exposure of the prescalene fat pad. A 4-to 5-cm skin incision is made parallel to and just above the clavicle, starting over the medial head of the sternocleidomastoid muscle. The platysma is divided, and the crossing external jugular vein is ligated. The posterior border of the clavicular head of the sternocleidomastoid is isolated, and the muscle is retracted. The jugular vein is isolated by blunt dissection with a mounted sponge or dissecting forceps. The inferior belly of the omohyoid muscle is identified at the level of the vascular sheath and retracted upward (Fig. 11.2). Mobilization of the prescalene fat pad. At this point the prescalene fat has been exposed between the jugular vein, clavicular margin, and omohyoid muscle. The deep cervical fascia is approached from the omohyoid by blunt dissection with two mounted sponges, and the fat–lymph node tissue is carefully dissected downward on the cervical fascia as far as the junction of the subclavian and jugular veins. The thyrocervical trunk is preserved. The deep cervical fascia should also be preserved to avoid injury to the phrenic nerve and brachial plexus (Fig. 11.3). Fig. 11.2 Scalene node biopsy, step 1. The skin is incised parallel to the clavicle. The external jugular vein (3) is ligated, and the clavicular head of the sternocleidomastoid muscle (2) and the inferior belly of the omohyoid muscle (1) are exposed. Fig. 11.3 Scalene node biopsy, step 2. The sternocleidomastoid and internal jugular vein are retracted medially, and the inferior belly of the omohyoid muscle is retracted upward. The prescalene fat is exposed into the angle of the jugular and subclavian veins. The phrenic nerve (3) and brachial plexus (2) must be preserved. (1) Transverse cervical artery, (4) scalene muscle. The drain is removed when the drainage volume falls to 30 mL or less. The Committee for Neck Dissection Classification of the American Head and Neck Society has issued a revised version of the cervical lymph node classification based on various discussions on regional definitions and the nomenclature of neck dissections. The lymph node groups are classified as follows: Lymph nodes omitted in this classification include: The current neck dissection classification published by Robbins (2002) still distinguishes among a radical neck dissection, extended radical neck dissection, modified radical neck dissection, and selective neck dissection. Radical neck dissection. A radical neck dissection involves the complete removal of levels I–V lymph nodes including all three major nonlymphatic structures—the accessory nerve, internal jugular vein, and sternocleidomastoid muscle. The resection does not include the suboccipital lymph nodes, periparotid lymph nodes, retropharyngeal lymph nodes, or anterior compartment lymph nodes (level VI). Extended radical neck dissection. An extended radical neck dissection consists of a radical neck dissection plus the removal of one or more additional lymph node groups and/or nonlymphatic structures such as the external carotid artery, hypoglossal nerve, vagus nerve, or paravertebral muscles. Modified radical neck dissection. This operation removes the level I–V lymph nodes in addition to one or more nonlymphatic structures (accessory nerve and/or internal jugular vein and/or sternocleidomastoid muscle). Selective neck dissection. This operation removes the lymph node levels that principally drain a malignant tumor of the upper aerodigestive tract while sparing all three major nonlymphatic structures. The classic types of selective neck dissection are designated I–III, I–IV, II–IV, and II–V. If only two levels are removed, the selective neck dissection is named accordingly (e. g., SND II–III). Radical neck dissection. In Europe and at most institutions, a radical neck dissection is reserved for the treatment of N3 metastasis or metastases that involve nonlymphatic structures. Modified radical neck dissection. Most head and neck surgeons currently perform a modified radical neck dissection in all patients with clinically detectable lymph node metastasis. There is a definite trend, however, toward sparing certain levels such as level IIB in hypopharyngeal carcinoma or level I for the same tumor entity. A bilateral modified radical neck dissection is performed in patients with an N2c neck, or bilateral lymphogenous metastasis. Every effort consistent with oncologic requirements should be made to preserve the internal jugular vein on at least one side of the neck to prevent potentially severe lymphedema. A selective neck dissection should be considered in patients with a contralateral N0 neck in consideration of the overall prognosis. Thus, an ipsilateral metastasis at level IV would be more detrimental to survival than a metastasis at level II. Some authors would advocate a selective neck dissection even in patients with an N+ status, but the validity of this policy has yet to be established. At this point we wish to provide the surgeon in training with some principles that may be followed for the oncologically sound surgical management of the clinical N0 neck. Table 11.1 lists types of selective neck dissection that are recommended for specific primary tumor sites in the upper aerodigestive tract. It is important to consider selection criteria for a bilateral selective neck dissection in the clinical N0 neck. The policy at many centers is to recommend this operation in cases where the primary tumor is located in the midline or has transgressed the midline. Of course, the table presents only one of several possible surgical strategies whose application will depend on the overall oncologic policy of the particular institution. En bloc resection of all cervical lymphatic tissue and fat at levels I–V in continuity with major nonlymphatic structures—the sternocleidomastoid muscle, internal jugular vein, and accessory nerve. By definition, this operation includes removal of the submandibular gland. Fixed cervical lymph node metastases, N3 metastases. Debilitated patient who is a poor candidate for surgery. Incurable primary tumor, incurable distant metastases, invasion of the carotid artery (relative contraindication, may be avoided by vascular grafting). Metastasis with contiguous invasion of prevertebral and nuchal soft tissues. Clinical N0 neck. B-mode ultrasonography and CT of the cervical soft tissues, plus thoracic CT to exclude distant metastases.
Perioperative Antibiotics for Soft-Tissue Surgery of the Head and Neck
Distinction between Septic and Aseptic Surgery
Spectrum of Infectious Organisms
Timing and Duration of Antibiotic Therapy
Treatment of Wound Infections
Surgery of the Lymph Nodes
Lymph Node Abscesses
Surgical Principle
Indications
Contraindications
Specific Points Regarding Informed Consent
 Sensory disturbances involving the neck or ear.
Sensory disturbances involving the neck or ear.
 Paralysis of the nerves supplying the trapezius, visceral muscles, diaphragm, lingual muscles, sublingual muscles, vocal cords, and facial muscles.
Paralysis of the nerves supplying the trapezius, visceral muscles, diaphragm, lingual muscles, sublingual muscles, vocal cords, and facial muscles.
 Hoarseness or voice loss.
Hoarseness or voice loss.
 Poor cosmetic result, excessive scarring.
Poor cosmetic result, excessive scarring.
 Possible need to extend the skin incision.
Possible need to extend the skin incision.
 Need for a second operation.
Need for a second operation.
 Mucosal injury, mediastinitis.
Mucosal injury, mediastinitis.
Operative Planning
Special Instruments
Anesthesia
Surgical Technique
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 Risks and Complications
Risks and Complications
Postoperative Care
Cervicofacial Lymphadenectomy
Surgical Principle
Indications
Specific Points Regarding Informed Consent
 Sensory disturbance involving the neck or ear.
Sensory disturbance involving the neck or ear.
 Growth lag of the skin flap.
Growth lag of the skin flap.
 Paralysis of the nerves supplying the trapezius, visceral muscles, diaphragm, lingual muscles, sublingual muscles, vocalis, and facial muscles.
Paralysis of the nerves supplying the trapezius, visceral muscles, diaphragm, lingual muscles, sublingual muscles, vocalis, and facial muscles.
 Hoarseness or voice loss.
Hoarseness or voice loss.
 Dyspnea, which may necessitate a tracheostomy tube.
Dyspnea, which may necessitate a tracheostomy tube.
 Poor cosmetic result, excessive scarring.
Poor cosmetic result, excessive scarring.
 Possible need to extend the skin incision.
Possible need to extend the skin incision.
 Mucosal injury, mediastinitis.
Mucosal injury, mediastinitis.
 Persistent drainage of lymphatic fluid.
Persistent drainage of lymphatic fluid.
Operative Planning
Anesthesia
Surgical Technique
 Management of Injury to Large Venous Vessels
Management of Injury to Large Venous Vessels
 Risks and Complications
Risks and Complications
 Various structures may be at risk, depending on the location of the lymph node:
Various structures may be at risk, depending on the location of the lymph node:
 Secondary infections, fistula formation due to incomplete removal of tuberculous lymph nodes. Postoperative bleeding, keloid formation.
Secondary infections, fistula formation due to incomplete removal of tuberculous lymph nodes. Postoperative bleeding, keloid formation.
 An extremely rare but potentially severe complication is to misidentify a carotid body tumor as a lymph node (differentiating signs: pulsations, transverse mobility on palpation with little or no vertical mobility). Careless dissection may result in massive bleeding with risk of carotid injury.
An extremely rare but potentially severe complication is to misidentify a carotid body tumor as a lymph node (differentiating signs: pulsations, transverse mobility on palpation with little or no vertical mobility). Careless dissection may result in massive bleeding with risk of carotid injury.
Postoperative Care
Scalene Node Biopsy
Surgical Principle
Indications
 Histological identification of inaccessible tumors, thoracic tumors, or tumors that have undergone intra-abdominal metastasis
Histological identification of inaccessible tumors, thoracic tumors, or tumors that have undergone intra-abdominal metastasis
 Exclusion of suspected sarcoidosis or tuberculosis, even in the absence of palpable lymphadenopathy
Exclusion of suspected sarcoidosis or tuberculosis, even in the absence of palpable lymphadenopathy
 Suspected Hodgkin or non-Hodgkin lymphoma
Suspected Hodgkin or non-Hodgkin lymphoma
 Unexplained lymph node enlargement in the omoclavicular triangle
Unexplained lymph node enlargement in the omoclavicular triangle
Contraindication
Anesthesia
Surgical Technique
 Risks and Complications
Risks and Complications
 With injury to the thoracic duct, immediately locate and ligate the duct using the microscope. A chyle fistula that is detected after surgery can be managed conservatively in most cases by closely monitoring the chyle volume and obtaining a blood count, chest radiographs, urinary status, liver function, electrolytes, and serum protein assays including serum albumin. Most low-output fistulas can be successfully managed by a diet of medium-chain triglycerides to reduce chyle production. Parenteral nutrition alone is no longer considered a cost-effective approach. Conservative treatment measures for chyle fistula should be limited to 30 days so that planned postoperative radiotherapy can be instituted within a reasonable time frame. Chyle fistulas should be surgically repaired in patients with refractory hypoalbuminemia or if the fistula output is greater than 600 mL/24 hour.
With injury to the thoracic duct, immediately locate and ligate the duct using the microscope. A chyle fistula that is detected after surgery can be managed conservatively in most cases by closely monitoring the chyle volume and obtaining a blood count, chest radiographs, urinary status, liver function, electrolytes, and serum protein assays including serum albumin. Most low-output fistulas can be successfully managed by a diet of medium-chain triglycerides to reduce chyle production. Parenteral nutrition alone is no longer considered a cost-effective approach. Conservative treatment measures for chyle fistula should be limited to 30 days so that planned postoperative radiotherapy can be instituted within a reasonable time frame. Chyle fistulas should be surgically repaired in patients with refractory hypoalbuminemia or if the fistula output is greater than 600 mL/24 hour.
 If the pleura has been opened, the wound edges should be carefully reapproximated and secured with sutures. A suction drain is inserted if necessary, and surgical consultation should be sought.
If the pleura has been opened, the wound edges should be carefully reapproximated and secured with sutures. A suction drain is inserted if necessary, and surgical consultation should be sought.
 Injuries to the subclavian artery and vein are surgically repaired.
Injuries to the subclavian artery and vein are surgically repaired.
 Injuries to the phrenic nerve or brachial plexus are referred for neurosurgical repair.
Injuries to the phrenic nerve or brachial plexus are referred for neurosurgical repair.
 Other risks are keloid formation and secondary infection.
Other risks are keloid formation and secondary infection.
Postoperative Care
Neck Dissection
General
 Submental group (level IA).
Submental group (level IA).
 Submandibular group (level IB).
Submandibular group (level IB).
 Upper jugular group (level II), which is subdivided by the oblique accessory nerve into level IIA (lymph node-bearing fat above the accessory nerve) and level IIB (lymph node-bearing fat below the accessory nerve).
Upper jugular group (level II), which is subdivided by the oblique accessory nerve into level IIA (lymph node-bearing fat above the accessory nerve) and level IIB (lymph node-bearing fat below the accessory nerve).
 Middle jugular group (level III).
Middle jugular group (level III).
 Lower jugular group (level IV).
Lower jugular group (level IV).
 Posterior triangle group (level V). An imaginary horizontal line at the level of the cricoid cartilage subdivides this group into level VA (lymph node-bearing fat above the imaginary line) and level VB (lymph node-bearing fat below the imaginary line).
Posterior triangle group (level V). An imaginary horizontal line at the level of the cricoid cartilage subdivides this group into level VA (lymph node-bearing fat above the imaginary line) and level VB (lymph node-bearing fat below the imaginary line).
 Anterior compartment group (level VI).
Anterior compartment group (level VI).
 The retroauricular lymph nodes.
The retroauricular lymph nodes.
 The suboccipital lymph nodes.
The suboccipital lymph nodes.
 The parotid lymph nodes.
The parotid lymph nodes.
 The retropharyngeal lymph nodes.
The retropharyngeal lymph nodes.
Indications for Neck Dissection in the Treatment of Head and Neck Malignancies
Radical Neck Dissection
Surgical Principle
Indications
Contraindications
Specific Points Regarding Informed Consent
 Sensory disturbances involving the neck or ear.
Sensory disturbances involving the neck or ear.
 Growth lag of the skin flap.
Growth lag of the skin flap.
 Paralysis of the nerves supplying the trapezius, visceral muscles, diaphragm, lingual muscles, sublingual muscles, vocal and facial muscles.
Paralysis of the nerves supplying the trapezius, visceral muscles, diaphragm, lingual muscles, sublingual muscles, vocal and facial muscles.
 Hoarseness or voice loss.
Hoarseness or voice loss.
 Dyspnea, which may necessitate a tracheostomy tube.
Dyspnea, which may necessitate a tracheostomy tube.
 Poor cosmetic result, excessive scarring.
Poor cosmetic result, excessive scarring.
 Possible need to extend the skin incision.
Possible need to extend the skin incision.
 Mucosal injury, mediastinitis.
Mucosal injury, mediastinitis.
 Persistent discharge of lymphatic fluid.
Persistent discharge of lymphatic fluid.
 Lymphedema.
Lymphedema.
 Shoulder–arm syndrome.
Shoulder–arm syndrome.
 Limitation of motion by scar adhesions.
Limitation of motion by scar adhesions.
Operative Planning
Primary tumor site | Levels removed Classic SND |
More limited approach |
Upper lip | I–III + parotid lymph nodes | IB–II + parotid lymph nodes |
Lower lip | I–III | I–II |
Floor of mouth | I–III | I, II |
Mobile tongue | I–IV | I–II |
Soft palate | II–IV | II–III |
Tonsil | II–IV | II–III |
Tongue base | II–IV | II–III |
Supraglottis | II–IV | IIA–III |
Glottis | II–IV | IIA–III |
Piriform sinus | II–IV | IIA–IV |
Posterior wall of pharynx | II–V | II–IV |
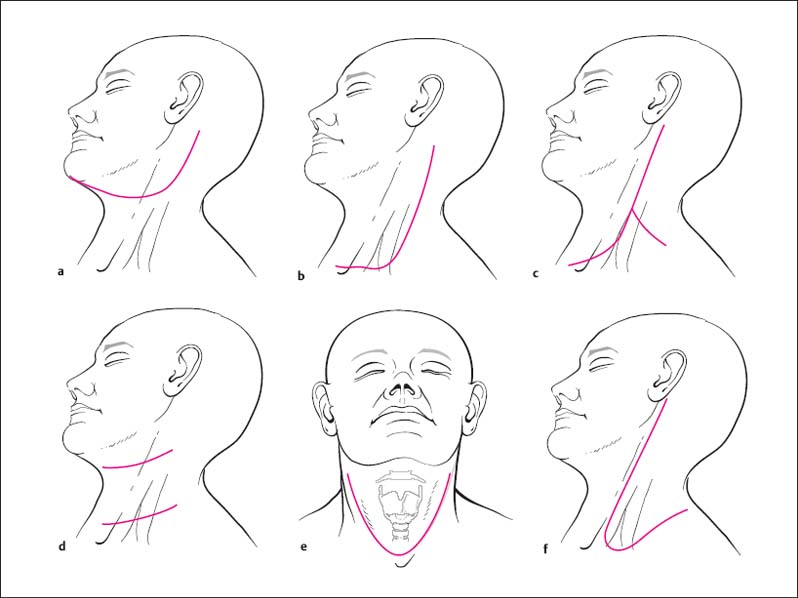
Fig. 11.4a–f Skin incisions for neck dissection.
a, e U-shaped incisions.
b, c Modified “hockey stick” incisions.
d MacFee incision.
f De Quervain incision.
Anesthesia
General endotracheal anesthesia.
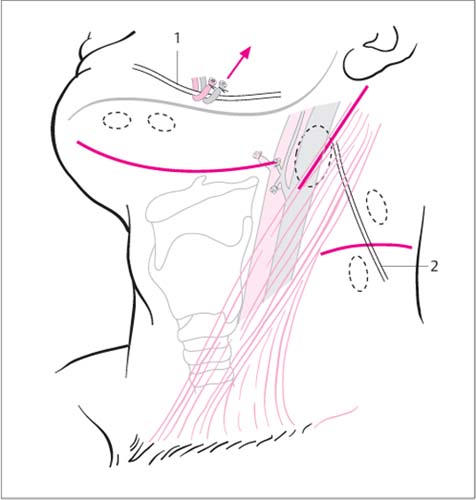
Surgical Technique
Skin incision. Key anatomic landmarks—the mandibular angle, the tip of the mastoid process, and the sternum—are first marked on the skin. The skin incision (Fig. 11.4) starts at the tip of the mastoid process and curves along the anterior border of the trapezius, passing two finger-widths above the clavicle and curving toward the sternum to terminate at the cervical midline.
Dissection of the skin flap. The first step after the skin incision is to elevate the skin flap. This is aided by constant tension applied by an assistant. The platysma is integrated into the skin flap to maintain an adequate blood supply to the flap. The flap can be developed with a scissors, scalpel, or electrocautery. A radical neck dissection will include resection of the external jugular vein, which may be ligated with absorbable suture material (2–0 Vicryl) or nonabsorbable material. By contrast, the internal jugular vein is always ligated with nonabsorbable suture material (e. g., 2–0 or 0 Mersilene) (Figs. 11.5 and 11.6).
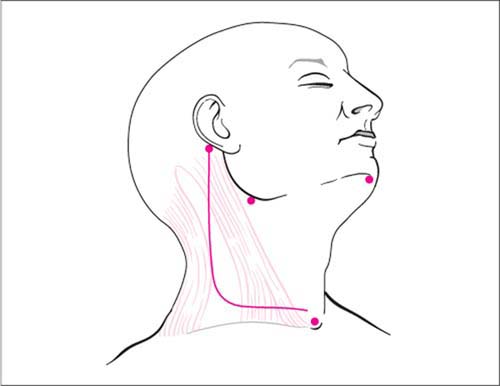
Fig. 11.5 Possible incision for radical neck dissection.
Key anatomic landmarks are marked on the skin before the incision is made.
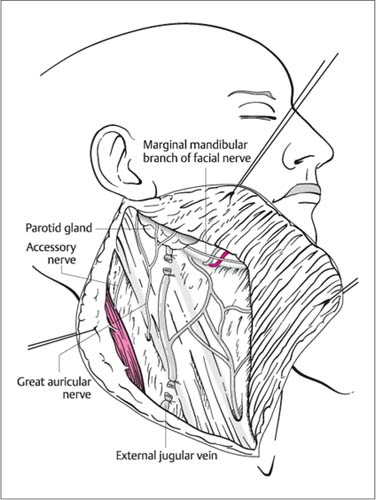
Fig. 11.6 Radical neck dissection.
The external jugular vein and its branches are incorporated into the surgical dissection.
Division of the great auricular nerve. The great auricular nerve is divided and the stumps cauterized with bipolar current to prevent neuroma formation. Dissection of the skin flap now continues toward the inferior pole of the parotid gland and the vertical ramus of the mandible, taking care to preserve the marginal branch of the facial nerve and the facial artery.
Fixation of the skin flap. The skin flap is retained by sutures to the surgical drapes.
Development of the inferior skin flap. The superficial fascia of the posterior triangle is incised and carefully spread open to expose the fatty tissue bearing the level V lymph nodes. The superficial fibers of the accessory nerve will enter the operative field during this part of the dissection. Because the accessory nerve may be sacrificed in a radical neck dissection, no special care is taken to preserve its superficial fibers. The inferior skin flap should be dissected to the anterior border of the trapezius muscle.
Dissection of level I nodes and the submandibular gland. The marginal branch of the facial nerve is at risk during resection of the level I nodes and submandibular gland. Generally this nerve branch crosses over the facial vein and artery at the approximate level of the inferior mandibular border (Fig. 11.7). The nerve branch should be identified at that location and traced a short distance posteriorly so that it can be safely mobilized upward from the field. Generally the facial vein is ligated. The hypoglossal nerve is exposed by elevating the intermediate tendon of the digastric muscle, whose course is traced cephalad. The hypoglossal nerve branch passing to the ansa cervicalis is ligated at the level where it crosses both carotid arteries. The dissection proceeds along the mandible to the submental attachment of the anterior belly of the digastric. The soft tissue between the anterior belly of the digastric and the mandible is mobilized. The dissection proceeds from the submental area across the anterior belly of the digastric to the midline raphe of the mylohyoid muscle, then continues on the mylohyoid to the free posterior border of that muscle. This requires a progressive posterior mobilization of the submandibular gland while identifying the excretory duct of the submandibular gland and the lingual nerve. Next, the submandibular (Wharton) duct is ligated with nonabsorbable 2–0 suture material (e. g., Mersilene). Care is taken to preserve the lingual nerve and the hypoglossal nerve, which runs from anterior to posterior in the adjacent fat. The hypoglossal nerve runs across the hyoglossus muscle, deep to the intermediate tendon of the digastric and behind the submandibular duct. When mobilization is completed, the submandibular gland can be separated from the facial artery in continuity with the surrounding lymph node-bearing soft tissue and reflected downward into the neck dissection specimen.
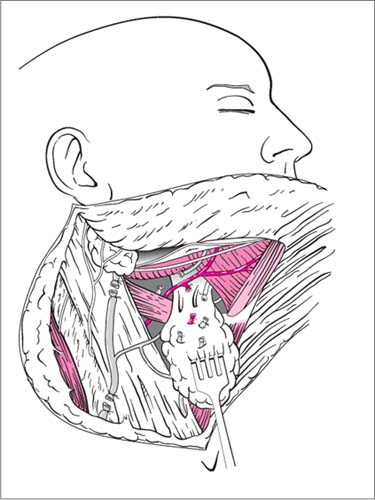
Fig. 11.7 Radical neck dissection.
The level I dissection includes removal of the submandibular gland. Nerves in that region are preserved.
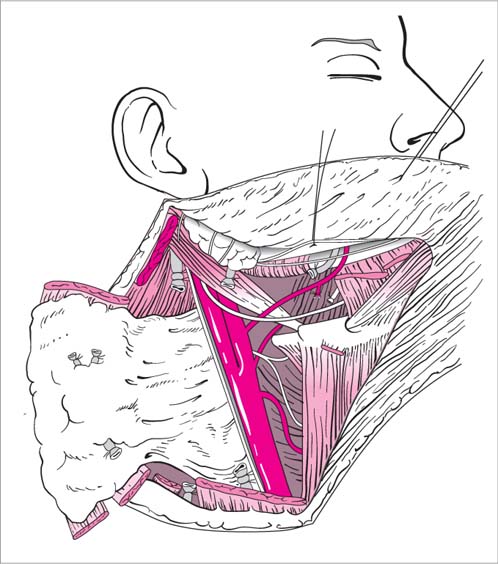
Fig. 11.8 Radical neck dissection.
Levels I–IV have been removed.
Dissection of levels II–IV. The sternocleidomastoid muscle is progressively detached in a lateral-to-medial direction (e. g., with an electrocautery) until all its fiber bundles have been released (Fig. 11.8
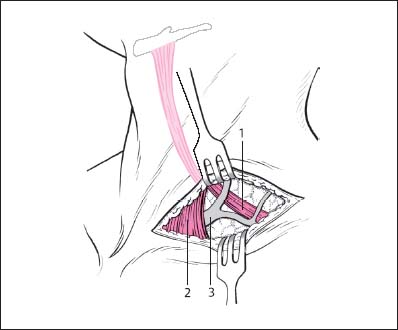
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


