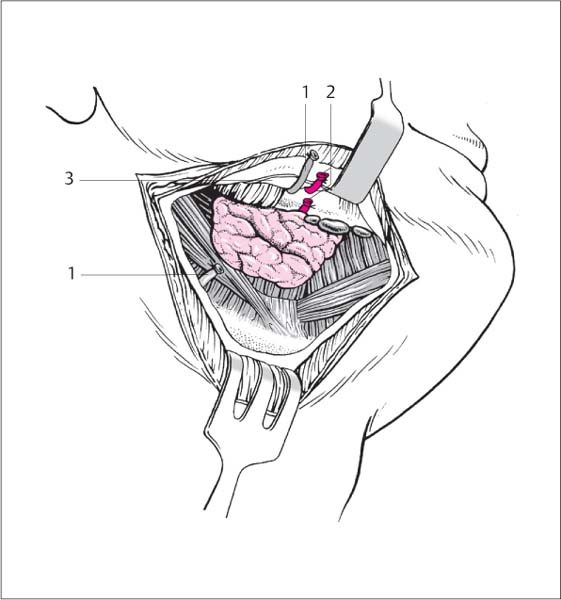
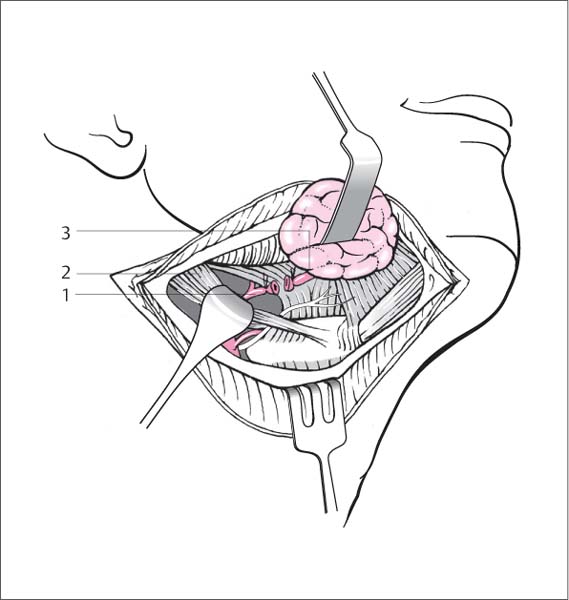
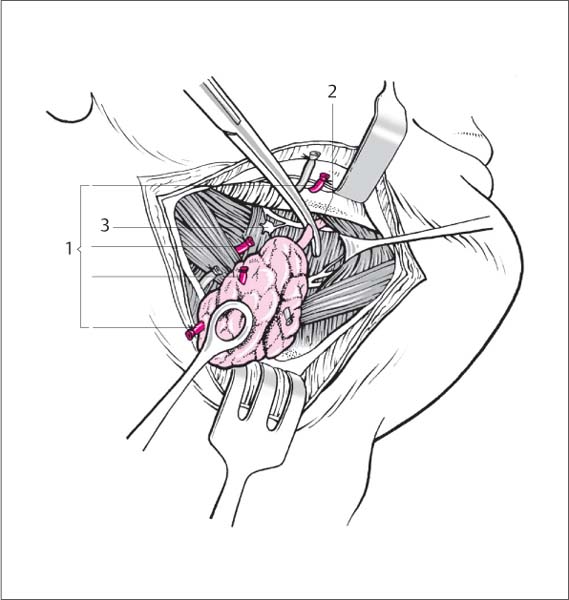
13 Surgery of the Salivary Glands Incision of the duct from the caruncle or over the stone, followed by extraction of the stone. Stones in the distal excretory duct. The stone is identified and localized by palpation and ultra-sonography. Plain radiographs or sialography may be necessary in some cases. CT scans are rarely required. Blunt-tipped scissors for incising the duct. Salivary duct probes or dilators may be required. Microscope or binocular loupe. Topical anesthesia followed by infiltration with a local anesthetic containing epinephrine. Incision. A probe or dilator is introduced into the caruncle under microscopic vision. The lower blade of a blunt-tipped scissors is inserted, and the overlying tissue is incised to the stone. Another techniquae is to incise the mucosa directly over the stone and spread the tissue apart to expose the duct, which is incised on the stone (Fig. 13.1). Extraction. The stone is easily shelled out with a small hook advanced to a point behind the stone. It may also be helpful to use a slender suction tip to retrieve a stone near the hilum without extensive tissue division. External pressure on the gland will keep the stone from receding. None of the incisions are sutured. Sialendoscopy has meanwhile achieved a high clinical relevance. Hereby a thin sialendoscope is inserted into the duct system (submandibular gland and parotid gland), the lesion is diagnosed, and even interventions can be performed such as transsections of synechia, stone extraction, etc. Fig. 13.1 Incision of the submandibular duct. One blade of a blunt-ended scissors is introduced into the duct from the caruncle, and the intervening tissue is divided. Antibiotic therapy. Complete removal of the submandibular gland from the neck while preserving the marginal mandibular branch of the facial nerve. General anesthesia is preferred. Standard neck tray. Incision. A curved incision ca. 4–5 cm long is made two finger-widths below the mandible, extending to the anterior border of the sternocleidomastoid muscle. The fat and platysma are divided in a strictly perpendicular plane (Fig. 13.2). Exposure of the gland. The superficial cervical fascia deep to the platysma is spread apart at a relatively low level. The facial vein in the posterior part of the field is isolated, ligated, and reflected upward. The fascia and vessel are bluntly dissected upward to the mandibular border, proceeding directly on the gland surface. The facial artery is usually encountered at this point; it is bluntly isolated on the gland, doubly ligated, and reflected upward. This maneuver also retracts the marginal mandibular branch of the facial nerve, which crosses over both vessels, out of the operative field (Fig. 13.3). Mobilization. The gland is mobilized from its compartment from the posterior side. The tissue at the posterior border is spread open and the cavity bluntly deepened with two mounted sponges, exposing the proximal portion of the facial artery in front of the posterior belly of the digastric. If the vessel enters the gland, it is doubly ligated and divided (Fig. 13.4). At this point the body of the gland can be freed from its compartment from the posterior aspect. The hypoglossal nerve is visible above the digastric loop in the deeper portion of the field. Smaller veins can now be accurately identified and ligated. Anterior mobilization. The anterolateral pole of the gland that overlies the mylohyoid muscle is bluntly mobilized. The part of the gland that extends medially forward around the edge of the mylohyoid muscle is freed with a dissecting forceps while several veins are coagulated. Division of the duct. At this point the gland is still attached by its excretory duct, and it is attached by the submandibular ganglion to the lingual nerve, which runs deeply parallel to the duct. With traction on the gland, the submandibular ganglion is transected and the lingual nerve is bluntly retracted. The duct is doubly ligated and divided, and the gland is removed (Fig. 13.5). Fig. 13.2 Excision of the submandibular gland. The skin is incised two finger-widths below the mandible. Fig. 13.3 Excision of the submandibular gland. The facial vein (1) is ligated and reflected upward. The facial artery (2) is also ligated at the superior border of the gland, below the mandible, and reflected upward. Both superior vascular stumps hold the marginal mandibular branch of the facial nerve out of the operative field (3). Fig. 13.4 Excision of the submandibular gland. The proximal facial artery (1) is ligated above the posterior belly of the digastric muscle (2) before it enters the gland (3). Fig. 13.5 Excision of the submandibular gland. 1 Vascular stumps of the facial artery 2 Division of the duct 3 Submandibular ganglion Wound closure. The wound is closed in layers over a suction drain. The suction drain is removed according to drainage volume. Antibiotic coverage is indicated perioperatively or if signs of inflammation appear. Lithiasis can be treated by duct incision, basket extraction, or lithotripsy. Increasing application of interventionl sialendoscopy. The most frequent surgical intervention refers to the treatment of the ranula that allows several therapeutic options, such as complete extirpation, sometimes also broad marsupialization. In each case, special attention must be paid to the lingual nerve, which must always be identified and preserved in surgery of the lateral floor of the mouth. Injuries of the parotid gland may be superficial with a parenchymal fistula, may involve ductal injury, or may be deep with associated profuse arterial bleeding and facial nerve disruption. Superficial injuries are treated by accurate suture re-approximation of the parenchymal lesion. The repair should include the parotid capsule, which is accurately closed with a purse-string suture or continuous plicating suture depending on the location and pattern of the injury. If salivation returns and atropine administration does not relieve salivary pressure on the suture line, the repair will have to be repeated. The extensive destruction of parotid tissue is managed by parotidectomy with preservation or reconstruction of the facial nerve. Reconstruction of the parotid (Stenson) duct over a catheter stent. Fresh injury of the excretory duct outside the parotid gland. Intraglandular duct injury or extensive glandular injury (an indication for parotidectomy). Microscope, salivary duct catheter made of vinyl or silicone. Local or general anesthesia. After the wound has been cleaned and the wound edges debrided, a catheter is inserted into the excretory duct from the buccal side. The appearance of the catheter in the wound serves to identify the distal limb of the parotid duct. The operating microscope is brought to bear, and the proximal duct stump is identified by salivary discharge during milking of the duct. The proximal stump is also threaded onto the catheter and re-approximated to the distal stump with micro-sutures. The wound is closed. Obtain meticulous hemostasis after identifying the duct. Firmly retract and expose the cut surface to help identify the duct. Facial nerve injury, infection, stricture, cutaneous salivary fistula in the cheek. Extensive injuries or inability to locate the proximal duct stump will necessitate a parotidectomy with facial nerve dissection. If a buccal fistula develops as a late sequela, the fistula should be outlined with an elliptical incision. The attached fistula tract is mobilized, drawn into a mucosal incision and sutured there. Another option is parotidectomy. Reconstruct the nerve by performing an end-to-end anastomosis or interposing a nerve graft.
Surgery of the Submandibular Salivary Gland
Incision of the Submandibular Duct
Surgical Principle
Indication
Contraindications
 Intraglandular stones.
Intraglandular stones.
 Recurrent multiple lithiasis.
Recurrent multiple lithiasis.
 Reactive chronic inflammatory glandular changes following prolonged stone obstruction or sialadenitis.
Reactive chronic inflammatory glandular changes following prolonged stone obstruction or sialadenitis.
Specific Points Regarding Informed Consent
 High incidence of recurrence.
High incidence of recurrence.
 Salivary stasis due to duct stricture.
Salivary stasis due to duct stricture.
 Wound infection.
Wound infection.
 Numbness due to lingual nerve injury.
Numbness due to lingual nerve injury.
Operative Planning
Special Instruments
Anesthesia
Surgical Technique
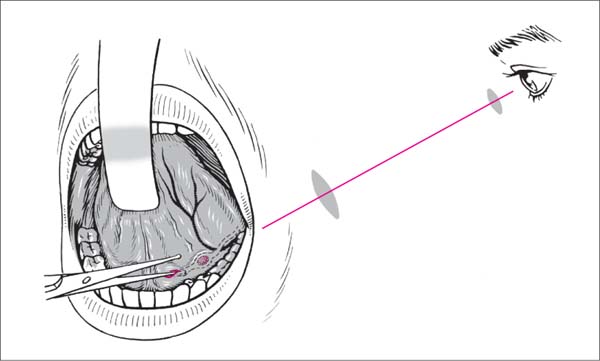
 The lingual nerve crosses beneath the submandibular duct near the gland and runs anteromedial to the excretory duct. To protect the nerve, incise only the tissue perpendicular or just lateral to the duct rather than near the hilum.
The lingual nerve crosses beneath the submandibular duct near the gland and runs anteromedial to the excretory duct. To protect the nerve, incise only the tissue perpendicular or just lateral to the duct rather than near the hilum.
 Distal stones require splitting the duct, while more proximal stones can be removed through an incision directly over the stone.
Distal stones require splitting the duct, while more proximal stones can be removed through an incision directly over the stone.
 Risks and Complications
Risks and Complications
 Sensory disturbances due to lingual nerve injury.
Sensory disturbances due to lingual nerve injury.
 Duct obstruction due to stricture or stenosis.
Duct obstruction due to stricture or stenosis.
 Occasional cellulitic inflammation of the oral floor.
Occasional cellulitic inflammation of the oral floor.
Postoperative Care
Alternatives
 Excision of the submandibular gland.
Excision of the submandibular gland.
 Lithotripsy.
Lithotripsy.
 Basket extraction.
Basket extraction.
 Sialendoscopy.
Sialendoscopy.
Excision of the Submandibular Gland
Surgical Principle
Indications
 Chronic recurrent submandibular sialadenitis.
Chronic recurrent submandibular sialadenitis.
 Recurrent sialolithiasis or intraglandular stone formation.
Recurrent sialolithiasis or intraglandular stone formation.
 Benign and malignant tumors of the submandibular gland.
Benign and malignant tumors of the submandibular gland.
 Part of a regional neck dissection.
Part of a regional neck dissection.
Contraindications
 Severe systemic disease.
Severe systemic disease.
 Massive, acute sialadenitis with cellulitis. Surgery is indicated only after unsuccessful antibiotic therapy or previous incision.
Massive, acute sialadenitis with cellulitis. Surgery is indicated only after unsuccessful antibiotic therapy or previous incision.
Specific Points Regarding Informed Consent
 Wound infection.
Wound infection.
 Injury to the marginal mandibular branch of the facial nerve with associated sensory disturbances.
Injury to the marginal mandibular branch of the facial nerve with associated sensory disturbances.
 Rare instances of lingual or hypoglossal nerve palsy with associated sensory or motor deficits.
Rare instances of lingual or hypoglossal nerve palsy with associated sensory or motor deficits.
 Postoperative bleeding, possibly associated with laryngeal edema or hematoma.
Postoperative bleeding, possibly associated with laryngeal edema or hematoma.
Operative Planning
 Palpation, especially bimanual.
Palpation, especially bimanual.
 Ultrasonography.
Ultrasonography.
 If necessary: sialography, CT, or MRI.
If necessary: sialography, CT, or MRI.
Anesthesia
Special Instruments
Surgical Technique
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 The marginal mandibular branch of the facial nerve can be directly identified and protected by facial nerve monitoring. This is safer than reflecting the nerve branch upward with the vascular stumps. The tissue above the ligated facial vein is explored with a stimulating electrode, and the nerve is identified and protected by spreading through the tissue in the direction that the nerve is expected to run.
The marginal mandibular branch of the facial nerve can be directly identified and protected by facial nerve monitoring. This is safer than reflecting the nerve branch upward with the vascular stumps. The tissue above the ligated facial vein is explored with a stimulating electrode, and the nerve is identified and protected by spreading through the tissue in the direction that the nerve is expected to run.
 Indirect thermal injury is avoided by using only bipolar coagulation in proximity to neural structures.
Indirect thermal injury is avoided by using only bipolar coagulation in proximity to neural structures.
 The hypoglossal nerve is located below the gland and excretory duct. It is visible above the tendon of the digastric muscle.
The hypoglossal nerve is located below the gland and excretory duct. It is visible above the tendon of the digastric muscle.
 Stones from the hilar area may become displaced anteriorly into the duct during the dissection. In some cases they can be “milked” back into place, but otherwise the duct should be dissected further and, if necessary, resected through the oral cavity.
Stones from the hilar area may become displaced anteriorly into the duct during the dissection. In some cases they can be “milked” back into place, but otherwise the duct should be dissected further and, if necessary, resected through the oral cavity.
 Arterial vessels should be at least doubly ligated to prevent the slippage of ligatures. Suture ligation is preferred to prevent significant postoperative bleeding with risk of hematoma formation and laryngeal edema.
Arterial vessels should be at least doubly ligated to prevent the slippage of ligatures. Suture ligation is preferred to prevent significant postoperative bleeding with risk of hematoma formation and laryngeal edema.
 Risks and Complications
Risks and Complications
 Injury to the marginal mandibular branch of the facial nerve; sensorimotor disturbances due to hypoglossal or lingual nerve injury.
Injury to the marginal mandibular branch of the facial nerve; sensorimotor disturbances due to hypoglossal or lingual nerve injury.
 Scarring, keloid formation, possible hollowing of the submandibular contour.
Scarring, keloid formation, possible hollowing of the submandibular contour.
 Postoperative wound infection, postoperative bleeding from arterial and venous vessels necessitating reintervention; risk of edema at the laryngeal inlet.
Postoperative wound infection, postoperative bleeding from arterial and venous vessels necessitating reintervention; risk of edema at the laryngeal inlet.
Postoperative Care
Alternatives
Surgery of the Sublingual Gland
Surgery of the Parotid Gland
Treatment of Parotid Gland Injuries
Parotid Parenchymal Fistula
Injury to the Parotid Duct
Surgical Principle
Indication
Contraindications
Specific Points Regarding Informed Consent
 Risk of facial nerve injury.
Risk of facial nerve injury.
 Fistula formation.
Fistula formation.
 Stricture formation in the excretory duct with stasis and recurrent parotiditis.
Stricture formation in the excretory duct with stasis and recurrent parotiditis.
Special Instruments
Anesthesia
Surgical Technique
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 Risks and Complications
Risks and Complications
Postoperative Care
 Antibiotic therapy.
Antibiotic therapy.
 Leave the catheter indwelling for 2–3 weeks. Administer atropine as required.
Leave the catheter indwelling for 2–3 weeks. Administer atropine as required.
Alternatives
Facial Nerve Injury
Surgical Principle
Indication
 Rules, Tips, and Tricks
Rules, Tips, and Tricks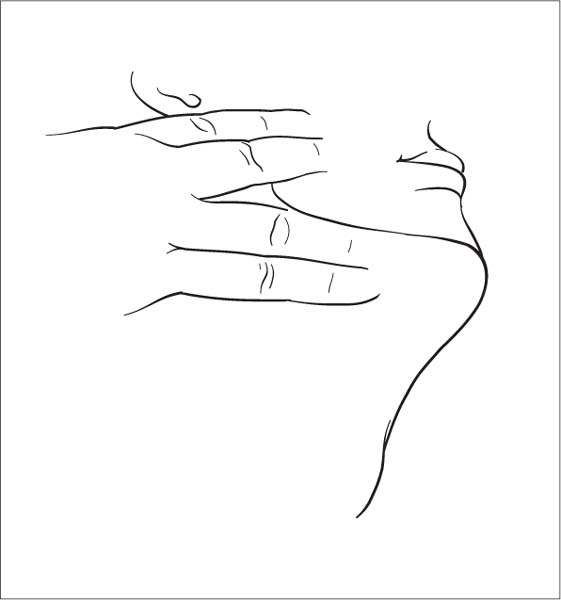
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


