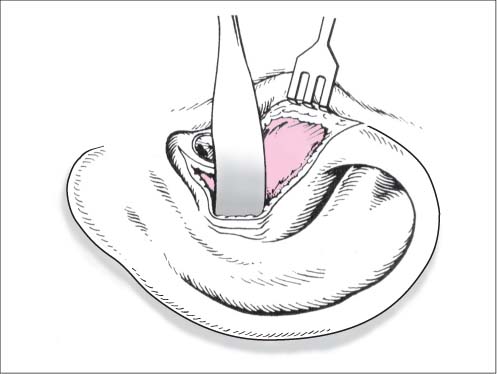
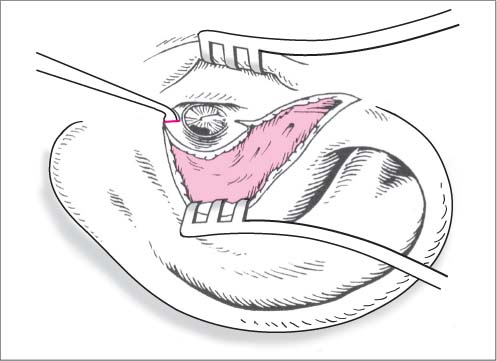
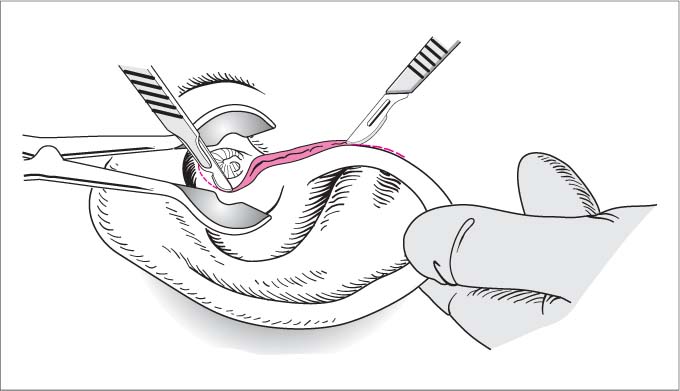
17 Surgical Approaches, Harvesting Grafts, and Implants The transcanal (endomeatal) approach to the tympanic membrane without incising the ear canal is adequate for myringotomies, tube insertions, and splinting tympanic membrane perforations. More extensive procedures require an endaural or postauricular approach to provide better visibility and access. Extended approach to the external ear canal, tympanic membrane, and middle ear by making an incision between the tragus and root of the helix. The endaural incision is also called the Heermann incision. Local anesthesia or general endotracheal anesthesia. Positioning. The patient is positioned supine on the operating table with the head turned to the side and immobilized on a headrest or ring. Exposure. The auricle is pulled upward and backward by an assistant. The meatal entrance is spread open with a nasal speculum. Incision. The first incision, made with a No. 10 or 15 blade, extends outward from the approximate center of the bony roof of the ear canal, initially keeping the blade in contact with the bone. It then follows the fissure between the tragal cartilage and root of the helix, which is easily visualized by adjusting the speculum tension, and runs parallel to the anterior helical rim. It may be only ca. 1 cm long (e. g., for stapes surgery) or may extend past the root of the helix, depending on the necessary degree of exposure. Temporalis fascia. When the incision reaches the end of the bony ear canal, it becomes more superficial and divides just the skin past that point, leaving the temporalis fascia and underlying muscle intact (Fig. 17.1). Next, the subcutaneous tissue and remaining connective tissue strands over the temporalis fascia and helix are mobilized by a combination of sharp and blunt dissection with a scissors, periosteal elevator, or scalpel. Meatal incision. The second, circumferential incision is made to the bone with a No.15 blade or round incision knife ca. 1 cm medial to the opening of the ear canal. It starts at the 6 o’clock position on the canal floor and circles upward to the 12 o’clock position on the posterior wall of the canal, where it meets the first incision at a right angle. Flap dissection. The triangular flap formed by the incisions is reflected laterally over the suprameatal spine with a periosteal elevator, keeping the blade in contact with the bone (Fig. 17.2). The self-retaining retractor blades are placed anteriorly and posteriorly, and if necessary a second endaural retractor can be placed at right angles to the first. Tympanomeatal flap. A tympanomeatal flap is outlined by making additional incisions toward the tympanic membrane at the 5 o’clock and 11 o’clock positions in the right ear or the 1 and 7 o’clock positions in the left ear (Fig. 17.3; see Rules, Tips, and Tricks below). Fig. 17.1 Endaural approach. The surgical site is exposed by inserting a speculum and pulling the auricle upward and backward. The first incision starts in the roof of the ear canal and runs outward, parallel to the root of the helix. The second, circumferential incision is made in the bony posterior wall of the ear canal ca. 1 cm from the meatal entrance. Fig. 17.2 Endaural approach. The posterior wall flap is mobilized over the suprameatal spine with a periosteal elevator. Fig. 17.3 Endaural approach. The tympanomeatal flap is created by making additional incisions at the 5 and 11 o’clock positions in the ear canal. A posterior incision is made around the root of the auricle, and the entrance to the ear canal is exposed. For a tympanoplasty, the ear canal is opened medial to the suprameatal spine. For a mastoidectomy, the periosteum over the mastoid cortex is divided and reflected from the bone.
Surgical Approaches
Endaural Approach
Surgical Principle
Indications
 Exostosis.
Exostosis.
 Circumscribed tumors of the ear canal.
Circumscribed tumors of the ear canal.
 Foreign body extraction.
Foreign body extraction.
 Stapes surgery.
Stapes surgery.
 Surgical correction of minor malformations.
Surgical correction of minor malformations.
 Tympanoscopy and second-look procedures.
Tympanoscopy and second-look procedures.
 Tympanoplasty without an extensive mastoidectomy.
Tympanoplasty without an extensive mastoidectomy.
Contraindications
 Mastoidectomy in patients with extensive pneumatization (relative), otogenic complications, or petrous bone fractures.
Mastoidectomy in patients with extensive pneumatization (relative), otogenic complications, or petrous bone fractures.
 Tympanoplasty for large cholesteatoma or poor visualization of lesions in the anterosuperior and inferior quadrants of a narrow, sharply angled ear canal (relative, depending on the surgeon’s experience).
Tympanoplasty for large cholesteatoma or poor visualization of lesions in the anterosuperior and inferior quadrants of a narrow, sharply angled ear canal (relative, depending on the surgeon’s experience).
Anesthesia
Surgical Technique
 Rules, Tips, and Tricks
Rules, Tips, and Tricks
 Do not incise the helical cartilage or temporalis fascia.
Do not incise the helical cartilage or temporalis fascia.
 Place the incision just anterior to the auricle to avoid damaging the superficial temporal artery and extensions from the superficial branch of the facial nerve.
Place the incision just anterior to the auricle to avoid damaging the superficial temporal artery and extensions from the superficial branch of the facial nerve.
 A narrow bony meatal entrance can be enlarged with a grinder or conical burr to create a funnel-shaped cavity.
A narrow bony meatal entrance can be enlarged with a grinder or conical burr to create a funnel-shaped cavity.
 If a bony overhang in the anterior canal wall is obscuring the anterior quadrants, it can be taken down with a diamond burr. First a U-shaped flap based on the tympanic membrane is cut over the prominence, dissected with a round knife to the tym-panic membrane annulus, and reflected onto the drum. The prominence is then burred down, and the flap is returned.
If a bony overhang in the anterior canal wall is obscuring the anterior quadrants, it can be taken down with a diamond burr. First a U-shaped flap based on the tympanic membrane is cut over the prominence, dissected with a round knife to the tym-panic membrane annulus, and reflected onto the drum. The prominence is then burred down, and the flap is returned.
 The distance of the circumferential incision from the tympanic annulus, and thus the length of the tympanomeatal flap, is variable. A longer (more laterally placed) flap incision is useful in cholesteatoma surgery for covering the bone defect in the posterior canal wall. A shorter flap (closer to the tympanic membrane) is better for a stapedectomy as it provides more space within the ear canal.
The distance of the circumferential incision from the tympanic annulus, and thus the length of the tympanomeatal flap, is variable. A longer (more laterally placed) flap incision is useful in cholesteatoma surgery for covering the bone defect in the posterior canal wall. A shorter flap (closer to the tympanic membrane) is better for a stapedectomy as it provides more space within the ear canal.
 If broad exposure of the mastoid is required, the skin incision can be extended upward and backward around the root of the helix into the postauricular sulcus. Before the incision is extended, the retractors should be loosened so that the cut can be continued in a straight line.
If broad exposure of the mastoid is required, the skin incision can be extended upward and backward around the root of the helix into the postauricular sulcus. Before the incision is extended, the retractors should be loosened so that the cut can be continued in a straight line.
 Risks and Complications
Risks and Complications
 Auricular perichondritis.
Auricular perichondritis.
 Injury of the parotid capsule.
Injury of the parotid capsule.
 Postoperative hemorrhage due to temporal artery injury.
Postoperative hemorrhage due to temporal artery injury.
 Special procedures are available for managing other complications.
Special procedures are available for managing other complications.
Postauricular Approach
Surgical Principle
Indications
 Tympanoplasty.
Tympanoplasty.
 Cholesteatoma removal.
Cholesteatoma removal.
 Antrotomy.
Antrotomy.
 Mastoidectomy, including treatment of otogenic complications.
Mastoidectomy, including treatment of otogenic complications.
 Saccotomy.
Saccotomy.
 Facial nerve decompression.
Facial nerve decompression.
 Translabyrinthine approach to the internal auditory canal.
Translabyrinthine approach to the internal auditory canal.
 Cochlear implant (modified approach, see Chapter 23).
Cochlear implant (modified approach, see Chapter 23).
 Implantable hearing aids.
Implantable hearing aids.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


