Purpose
To report refractive, topographic, aberrometric, and tomographic outcomes 24 months after corneal cross-linking (CXL) in patients up to 18 years of age with progressive keratoconus.
Design
Prospective, interventional case series.
Methods
Forty eyes underwent riboflavin-ultraviolet A-induced CXL. Uncorrected visual acuity (UCVA), best spectacle-corrected visual acuity (BSCVA), sphere and cylinder, topography, aberrometry, tomography, and endothelial cell counts were evaluated at baseline and at 1, 3, 6, 12, and 24 months.
Results
Mean logarithm of the minimum angle of resolution baseline UCVA and BSCVA were 0.79 ± 0.21 and 0.39 ± 0.10, respectively. Mean UCVA and BSCVA at 2 years were 0.58 ± 0.18 and 0.20 ± 0.09, respectively. The improvement in UCVA and BSCVA was significant throughout the postoperative follow-up ( P < .05). Mean spherical equivalent refraction showed a significant decrease of 1.57 diopters (D) at 24 months ( P = .02). Mean baseline simulated keratometry was 46.32 D in the flattest meridian and 51.48 D in the steepest meridian; at 2 years, the values were 45.30 D ( P = .04) and 50.21 D ( P = .07), respectively. For a 3-mm pupil, there was a significant reduction ( P < .05) in whole eye (total), corneal, higher-order, and astigmatic wavefront aberrations at 24 months. A significant difference ( P < .05) in total coma and total spherical aberration 2 years after CXL also was observed. Mean baseline pupil center pachymetry decreased significantly ( P = .04) at 6 months, but recovered by 12 months and remained stable thereafter through the 2-year follow-up. Endothelial cell counts did not change significantly ( P = .32).
Conclusions
CXL improved UCVA and BSCVA in the study patients, most likely by significantly reducing corneal asymmetry and corneal as well as total wavefront aberrations.
Keratoconus is a slowly progressive, noninflammatory corneal dystrophy characterized by changes in corneal collagen structure and organization. A reduced number of collagen cross-links and a pepsin digestion higher than normal have been suggested as possible explanations for an overall structural weakness of the corneal tissue in keratoconus, resulting in a stiffness that is only 60% of the normal cornea. Decreased mechanical corneal stability plays an important role in the progressive ectasia of the keratoconic cornea, resulting in mild to marked impairment of visual acuity resulting from irregular astigmatism, progressive myopia, corneal thinning, and central corneal scarring.
Progression of the disease can be dramatically faster in children, with increasing visual impairment, inability to obtain satisfactory correction with spectacles or soft contact lenses, and intolerance to rigid gas permeable contact lenses. Intracorneal ring segments implantation improves uncorrected visual acuity (UCVA) and best spectacle-corrected visual acuity (BSCVA) in patients with mild to moderate keratoconus and contact lens intolerance. However, long-term follow-up has shown that intracorneal ring segment implantation fails to provide a permanent flattening of the cornea. A significant progression of K-values in intracorneal ring segment-treated corneas has been observed, demonstrating that this procedure has only a temporary effect.
Collagen cross-linking (CXL) was introduced by Wollensak and associates to stabilize progressive keratoconus, to prevent some of the underlying pathophysiologic mechanisms of the disease, and to avoid the need for penetrating keratoplasty, which is usually required in advanced cases. The peer-reviewed literature, as well as our own experience with adult eyes that underwent CXL for progressive keratoconus and iatrogenic ectasia, demonstrated that the procedure was able to arrest progression. Further, no endothelial cell loss, no cataract development, and no permanent side effects were observed in the adults.
Accordingly, we initiated a CXL study in patients younger than 18 years with progressive stage II keratoconus (Amsler-Krumeich classification). In this cohort, we examined the refractive, topographic, aberrometric, and tomographic outcomes at 24 months after CXL.
Methods
Population
Forty eyes of 40 consecutive white patients (9 females, 31 males) in which keratoconus progression was observed in the preceding 3 months were enrolled at the Departments of Ophthalmology, Istituto Clinico Humanitas, Rozzano-Milano, Italy, and Inselspital University Hospital, Bern, Switzerland, in 2008 in this prospective, nonrandomized, study.
Preoperative keratoconus progression was confirmed by serial differential corneal topographies and by differential optical pachymetry analyses in all eyes included in the study. Keratoconus progression was defined as a change in either myopia or astigmatism of at least 3.0 diopters (D) in the previous 3 months, or a mean central K reading change of at least 1.5 D observed in 2 consecutive topographies during the preceding 3 months, or a mean central corneal thickness decrease of at least 5% in 3 consecutive tomographies performed in the previous 3 months. The Amsler-Krumeich classification was used for keratoconus grading. The corneal higher-order aberrations scale could not be used as a measure of progression because many ophthalmologists who referred patients for keratoconus progression did not provide aberration data.
Inclusion criteria were a documented keratoconus progression in the previous 3 months, corneal thickness of at least 400 μm at the thinnest point, and age up to 18 years. The age of the patients included in the study ranged from 9 to 18 years (mean, 14.2 ± 1.7 years). All treated eyes were graded stage II according to the Amsler-Krumeich classification.
Exclusion criteria included corneal thickness less than 400 μm at the thinnest point, a history of herpetic keratitis, severe dry eye, concurrent corneal infections, concomitant autoimmune diseases, and any previous ocular surgery. Also excluded were patients with central or paracentral corneal opacities, patients with poor compliance, and patients wearing rigid gas permeable lenses for at least 4 weeks before baseline examination.
At baseline and at each of the postoperative follow-up examinations (1, 3, 6, 12, and 24 months), all patients underwent UCVA and BSCVA assessment; slit-lamp biomicroscopy; basal Schirmer testing; Goldmann tonometry; dilated fundus examination; endothelial biomicroscopy (Konan Specular Microscope; Konan Medical Inc, Hyogo, Japan); corneal topography; corneal, internal, and total aberrometry with the Optical Path Difference Platform (OPD; NIDEK, Gamagori, Japan); and central pachymetry and optical tomography with the Pentacam HR (Oculus Inc, Lynnwood, Washington, USA).
Visual Acuity Assessment
Visual acuity was assessed with the Early Treatment Diabetic Retinopathy Study logarithm of the minimal angle of resolution charts (Lighthouse International, New York, New York, USA) based on the design suggested by Bailey and Lovie and incorporating the recommendations of the U.S. National Academy of Sciences–National Research Council. The chart was described in detail by Ferris and associates. Measurements were made with best correction after a noncycloplegic refraction at 4 m.
Corneal Topography
Topography was analyzed with the OPD unit. The OPD documented the 21 Klyce indices provided by the Corneal Navigator Topo-Classifier Map (OPD; NIDEK, Gamagori, Japan). In keratoconus diagnosis, the Navigator was found to be more specific and sensitive than the Rabinowitz-McDonnel test and also more specific and sensitive than central corneal power of more than 47.2 D or inferosuperior asymmetry of more than 1.4 D.
Wavefront Analysis
Total (corneal and internal) wavefront analysis was performed with the OPD-Scan, which provides an aberrometric analysis of the eye, decomposing whole eye (total) aberrations into corneal aberrations resulting from the anterior corneal surface and internal aberrations because of the posterior corneal surface, the anterior chamber, the lens, the vitreous body, and the retina.
Anterior Chamber Analysis
Anterior chamber analysis was performed with the Oculus Pentacam HR, which uses a rotating Scheimpflug camera. The analyses performed with the Pentacam included pupil center pachymetry and the pachymetry of the thinnest point of the cornea. The Pentacam also measured total and partial corneal volume, anterior chamber volume, and anterior chamber depth. Anterior and posterior elevation maps are derived by using a toric reference body, with calculations based on the central radii and the eccentricity of the keratometry measurements. The advantage of the toric reference shape is its good approximation to astigmatic corneas.
Endothelial Cell Count
Endothelial cell count was performed according to the method described by Prinz and associates.
Cross-Linking Procedure
Thirty minutes before the procedure, systemic pain medication was administered and pilocarpine 2% drops were instilled in the eye to be treated. CXL was performed under sterile conditions in the surgical suite. Children younger than 15 years of age had 1 parent attend the procedure.
After topical anesthesia with 2 applications of lidocaine 4% and oxybuprocaine hydrochloride 0.2% drops, the patient was draped, the ocular surface was rinsed with balanced salt solution, and a lid speculum was applied. The corneal epithelium was abraded in a central, 9-mm diameter area with the aid of an Amoils brush (Vision Technology Co Ltd, Seoul, Korea).
Before beginning ultraviolet A irradiation, Ricrolin (SOOFT, Montegiorgio, Italy), a photosensitizing riboflavin 0.1% solution (10 mg riboflavin-5-phosphate in 20% dextran-T-500) was applied onto the cornea every minute for 30 minutes to achieve adequate penetration of the solution. Using a slit lamp with the blue filter, the surgeon confirmed the presence of riboflavin in the anterior chamber before ultraviolet irradiation was started. The cornea was exposed to a ultraviolet source emanating from a solid-state device (CSO-VEGA X-linker; Scandicci, Firenze, Italy) that emits light at a wavelength of 370 ± 5 nm and an irradiance of 3 mW/cm 2 or 5.4 J/cm 2 . Exposure lasted for 30 minutes, during which time riboflavin solution again was applied, this time once every 5 minutes. The cropped light beam has a 7.5-mm diameter. A calibrated ultraviolet A meter (LaserMate-Q; Laser 2000, Wessling, Germany) was used before treatment to check the irradiance at a 1.0-cm distance. The CSO-VEGA laser emission probe has only 1 central light-emitting diode radiation source to be held 54 mm from the treated eye. Intraoperative pachymetry was performed throughout the procedure. Fixation during irradiation was achieved by instructing the patient to focus on the central LED of the probe. During the procedure, the surgeon also controlled for centration of treatment. Both topical anesthetics were added as needed during irradiation.
After surgery, patients received cyclopentolate (Ciclolux; Allergan, Roma, Italy) and levofloxacin drops (Oftaquix; Tubilux Pharma, Pomezia, Italy). A soft bandage contact lens was applied until re-epithelialization was complete. Topical levofloxacin was given 4 times daily for 7 days, dexamethasone 21-phosphate 0.15% drops (Etacortilen; Sifi, Lavinaio, Italy) were administered 3 times daily for 20 days, and sodium hyaluronate 0.15 % drops (BluYal; SOOFT) were applied 6 times daily for 45 days. In addition, patients received oral amino-acid supplements (Trium; SOOFT) for 7 days. Patients were examined daily until the epithelium healed.
Statistical Analysis
Statistical analyses were performed with the Statistica computer package (StatSoft Inc, Tulsa, Oklahoma, USA). All data are reported as mean ± standard deviation. Normality of the data was tested using the Wilcoxon test and was chi-square corrected with the Fisher test, when necessary. Comparisons were performed using the Student t test. The level of statistical significance was set at P < .05.
Results
Visual Acuity
UCVA and BSCVA data, expressed in logarithm of the minimal angle of resolution units and covering the entire follow-up period, are summarized in Figure 1 . Mean ± standard deviation (SD) baseline UCVA was 0.79 ± 0.21. Mean ± SD UCVA readings after CXL were as follows: 1 month after CXL, 0.69 ± 0.16; 3 months after CXL, 0.58 ± 0.20; 6 months after CXL, was 0.66 ± 0.17; 12 months after CXL, 0.62 ± 0.19; and at 24 months after CXL, 0.58 ± 0.18. Mean ± SD baseline BSCVA was 0.39 ± 0.10. Mean ± SD BSCVA readings after CXL were as follows: 1 month after CXL, 0.28 ± 0.13; 3 months after CXL, 0.25 ± 0.09; 6 months after CXL, 0.23 ± 0.11; 12 months after CXL, 0.21 ± 0.11; and 24 months after CXL, 0.20 ± 0.09.
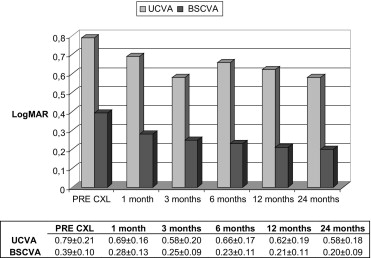
UCVA and BSCVA improvements were statistically significant ( P < .05) throughout the entire postoperative period when compared with the preoperative values. Both UCVA and BSCVA improved significantly during the first 6 months after CXL and remained unchanged between 6 and 24 months after surgery.
Refractive Results
The mean ± SD preoperative spherical equivalent was −3.63 ± 3.45 D, with a mean ± SD sphere of −2.32 ± 2.87 D and a mean ± SD cylinder of −2.87 ± 1.12 D. Two years after CXL, mean ± SD spherical equivalent was −2.06 ± 2.21 D, mean ± SD sphere was −1.38 ± 1.64 D, and mean ± SD cylinder was −1.56 ± 1.38 D. The difference in mean spherical equivalent was 1.57 D, a statistically significant reduction ( P = .02) because of a statistically significant decrease of both sphere ( P = .01) and cylinder ( P = .02). Vector analysis showed an axis shift from 100.72 ± 32.16 degrees to 110 ± 41.29 degrees after CXL, a difference that was not statistically significant ( P = .15).
Topographic Results
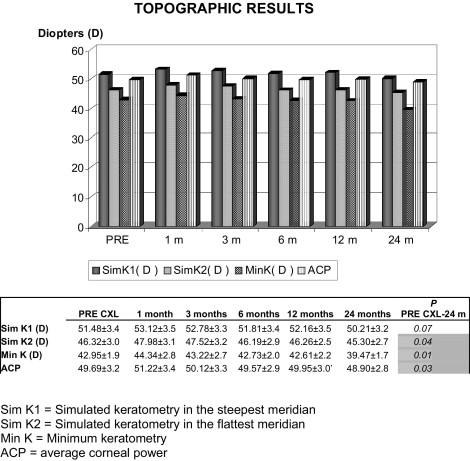
Topographic astigmatism measured with the OPD-Scan during follow-up is shown in Figure 2 . Mean baseline simulated keratometry 2, simulated keratometry 1, and minimum keratometry were 46.32 D, 51.48 D, and 42.95 D, respectively. At 24 months, these readings were 45.30 D, 50.21 D, and 39.47 D, respectively, a difference that was statistically significant for simulated keratometry 2 ( P = .04) and minimum keratometry ( P = .01). Mean average corneal power was 49.69 D at baseline and 48.90 D at 24 months, a difference that was statistically significant ( P = .03). These results demonstrate a flattening effect of CXL on the keratoconic cornea. The Klyce indices obtained with the OPD platform were analyzed at baseline and at 24 months ( Table 1 ).
| Before Cross-Linking | 1 Year after Cross-Linking | 2 Years after Cross-Linking | |
|---|---|---|---|
| Simulated keratometry in the steepest meridian (D) | 51.48 | 52.16 | 50.21 |
| Simulated keratometry in the flattest meridian (D) | 46.32 | 46.26 | 45.30 |
| Minimum keratometry (D) | 42.95 | 42.61 | 39.47 |
| Average corneal power (D) | 49.69 | 49.95 | 48.90 |
| Simulated keratometry cylinder (D) | 6.05 | 6.05 | 5.57 |
| Coefficient of variation of corneal power) a | 100.99 | 99.04 | 99.37 |
| Standard deviation of corneal power a | 4.97 | 4.78 | 4.8 |
| Corneal eccentricity index a | 1.05 | 0.9 | 0.84 |
| Logarithm of the minimal angle of resolution a | 0.29 | 0.28 | 0.27 |
| Differential sector index a | 11.10 | 11.20 | 12.05 |
| Surface regularity index a | 1.66 | 1.67 | 1.58 |
| Area compensated surface regularity index a | 1.46 | 1.48 | 1.44 |
| Surface asymmetry index a | 2.61 | 2.58 | 2.68 |
| Irregular astigmatism index a | 0.63 | 0.63 | 0.62 |
| Opposite sector index a | 8.87 | 8.81 | 9.41 |
| Center surround index a | 3.21 | 2.68 | 2.45 |
| Keratoconus index a | 0.79 | 0.75 | 0.74 |
| Keratoconus prediction index a | 0.41 | 0.39 | 0.40 |
| Elevation/depression power (D) | 3.69 | 3.88 | 3.64 |
| Elevation/depression diameter (mm) | 14.88 | 13.59 | 14.49 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


