51 Tumours of the Thyroid and Parathyroid Glands • Usually present as solitary nodule or dominant nodule in MNG • Middle-aged women • Not premalignant • Rarely become toxic • Encapsulated • Microscopic patterns: • Malignancy excluded by ruling out capsular or vascular invasion on histology • Family history of thyroid cancer • Exposure to ionizing radiation • 80% of thyroid malignancy • “Only” thyroid cancer in children • 5th decade • Presents as thyroid nodule • Microcarcinoma <1 cm diameter • Histological subtypes: • Psammoma bodies in fibrous stalk • Ground-glass “orphan Annie” nuclei • High incidence of LNs in levels III to VII (60%) • Primary tumour may be impalpable—therefore often presents with LNs • 20% have pulmonary mets at presentation • Bony mets less common • More aggressive in older age groups—may invade larynx/trachea • 10-year survival >90% • 6th decade • 20% of all thyroid malignancies • Decreasing incidence in endemic goitre areas • Commonly presents as solitary thyroid nodule • May present with mets—bone/lung in 20 to 30% • Non-vesicular nuclei • Histology required following surgical resection to determine diagnosis • Aka eosinophilic/oncocytic/oxyphilic cell • More aggressive variant of follicular ca (2% total) • Is possibly a degenerative/metaplastic phenomenon • Found in: • Malignant tumours display capsular and vascular invasion • May invade surrounding tissue and extrathyroid structures • LN mets common • 5% of all thyroid malignancies • May occur as part of MEN syndrome: • Bilateral in 90% of cases with MEN • LN mets in 25 to 30% • Arise from parafollicular/C cells • Calcitonin = tumour marker • Uniform spindle-shaped cells with variable fibrous stroma on histology • Account for <5% of all lymphoma • Classically rapidly increasing swelling in neck of an elderly woman • Immunocytochemistry needed to distinguish from anaplastic carcinoma • Usually arises on background of chronic autoimmune thyroiditis • Most are high-grade B-cell NHL • Mostly stage I or II • Occasionally thyroid involved in widespread systemic lymphoma • Elderly women • Often long-standing enlargement of thyroid • Rapid increase in size associated with pain referred to ear and hoarseness ± airway obstruction • Aggressively malignant with high metastatic potential • Commonly invade surrounding structures • Most patients dead within 1 year of presentation • Kidney and breast • CXR • USS • CT scan • MRI scan • Scintigraphy • TFTs—mandatory • Thyroid autoantibodies • The British Thyroid Association (Guidelines 2007) recommend either use of TNM staging or MACIS systems to determine when a patient is low risk or high risk for recurrence. • TNM: Tumour size, node metastases, and distant metastases • MACIS: Metastases, age at presentation, completeness of surgical resection, invasion (extra thyroidal), size • Age > 45 years • Male
51.1 Benign Tumours
 Follicular
Follicular
 Microfollicular
Microfollicular
 Hürthle cell
Hürthle cell
 Embryonal
Embryonal
51.2 Malignancy Risk Factors
51.3 Malignant Tumours
51.3.1 Papillary Adenocarcinoma
 Pure papillary
Pure papillary
 Mixed papillary–follicular (most common)
Mixed papillary–follicular (most common)
 Follicular
Follicular
51.3.2 Follicular Adenocarcinoma
51.3.3 Hürthle Cell Tumours
 Nodular goitres
Nodular goitres
 Chronic lymphocytic thyroiditis
Chronic lymphocytic thyroiditis
 Diffuse toxic goitre
Diffuse toxic goitre
 Post-radiation
Post-radiation
 Post-chemotherapy
Post-chemotherapy
 Aging thyroids
Aging thyroids
51.3.4 Medullary Thyroid Carcinoma
 MEN IIA
MEN IIA
 MEN IIB
MEN IIB
 Familial non-MEN
Familial non-MEN
 Sporadic
Sporadic
51.3.5 Lymphoma
51.3.6 Anaplastic Cancers
51.3.7 Metastatic Deposits
51.4 Radiology
 Tracheal deviation
Tracheal deviation
 Mediastinal extension/LNs
Mediastinal extension/LNs
 Pulmonary mets
Pulmonary mets
 Co-morbidity
Co-morbidity
 Tumour size
Tumour size
 Diagnosing MNGs
Diagnosing MNGs
 Excludes contralateral disease
Excludes contralateral disease
 Evaluate complex cysts
Evaluate complex cysts
 Fine calcification 85 to 95% specific for papillary thyroid ca
Fine calcification 85 to 95% specific for papillary thyroid ca
 Combined with FNA for initial diagnosis
Combined with FNA for initial diagnosis
 Evaluate metastatic neck disease if suspected combined with FNA and thyroglobulin washout
Evaluate metastatic neck disease if suspected combined with FNA and thyroglobulin washout
 Avoid the use of iodinated contrast media when performing CT scans. This may reduce the subsequent radioiodine uptake by thyroid tissue and therefore delay its use
Avoid the use of iodinated contrast media when performing CT scans. This may reduce the subsequent radioiodine uptake by thyroid tissue and therefore delay its use
 Assess extent of larger tumours including larynx/trachea/oesophagus/major vessels
Assess extent of larger tumours including larynx/trachea/oesophagus/major vessels
 Demonstrates nodal deposits in neck/mediastinum
Demonstrates nodal deposits in neck/mediastinum
 Direct retrosternal extension
Direct retrosternal extension
 Pulmonary mets
Pulmonary mets
 Assess possible vessel involvement (MR angiography)
Assess possible vessel involvement (MR angiography)
 No contrast required
No contrast required
 Poorly specific and sensitive
Poorly specific and sensitive
 Technetium-99m mostly used due to cost and availability
Technetium-99m mostly used due to cost and availability
 90% of nodules are cold
90% of nodules are cold
 20% risk of malignancy in a cold nodule (50% if cyst excluded on USS)
20% risk of malignancy in a cold nodule (50% if cyst excluded on USS)
 Hot nodules unlikely to be malignant
Hot nodules unlikely to be malignant
 123I-MIBG used for suspected MEN
123I-MIBG used for suspected MEN
 131I radioiodine used for post-operative ablation and to search for mets
131I radioiodine used for post-operative ablation and to search for mets
51.5 Laboratory Investigations
 May assist diagnosis of chronic lymphocytic thyroiditis
May assist diagnosis of chronic lymphocytic thyroiditis
 Predict post-operative hypothyroidism
Predict post-operative hypothyroidism
 Helps interpretation of thyroid function and thyroglobulin
Helps interpretation of thyroid function and thyroglobulin
 Preop thyroglobulin not helpful
Preop thyroglobulin not helpful
 Serum calcium and calcitonin—if medullary ca suspected
Serum calcium and calcitonin—if medullary ca suspected
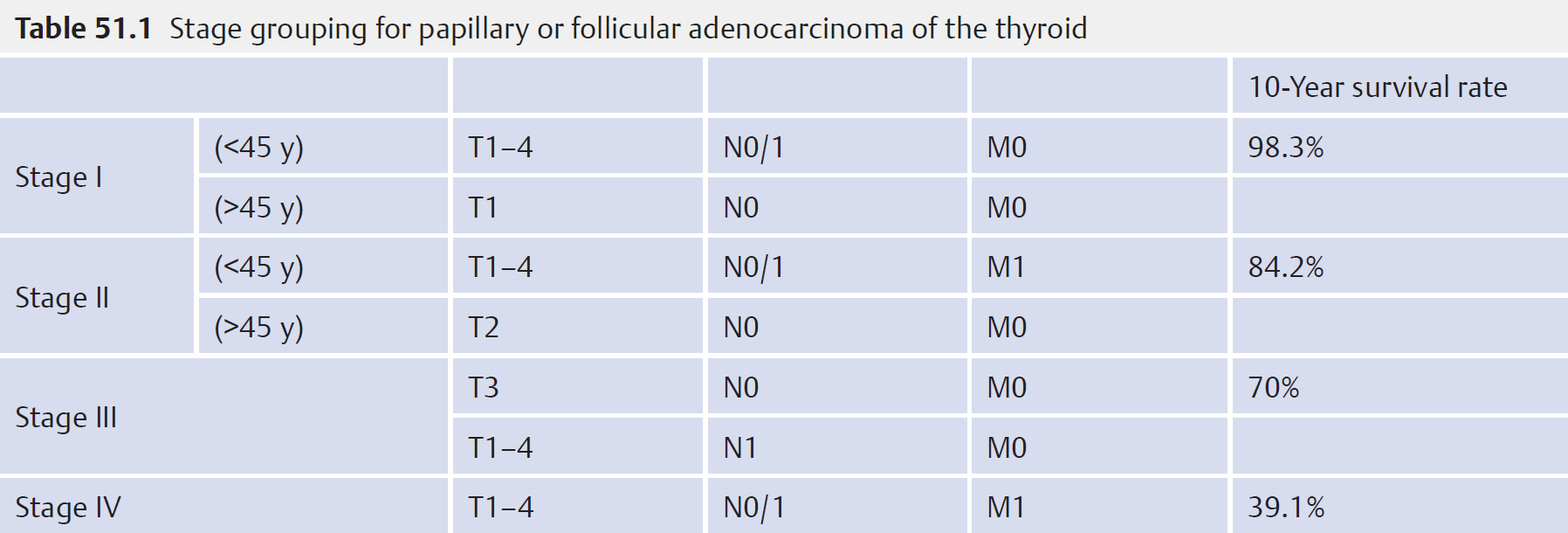
51.5.1 Prognostic Factors
51.6 Poor Prognostic Factors for DTC
< div class='tao-gold-member'>
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


