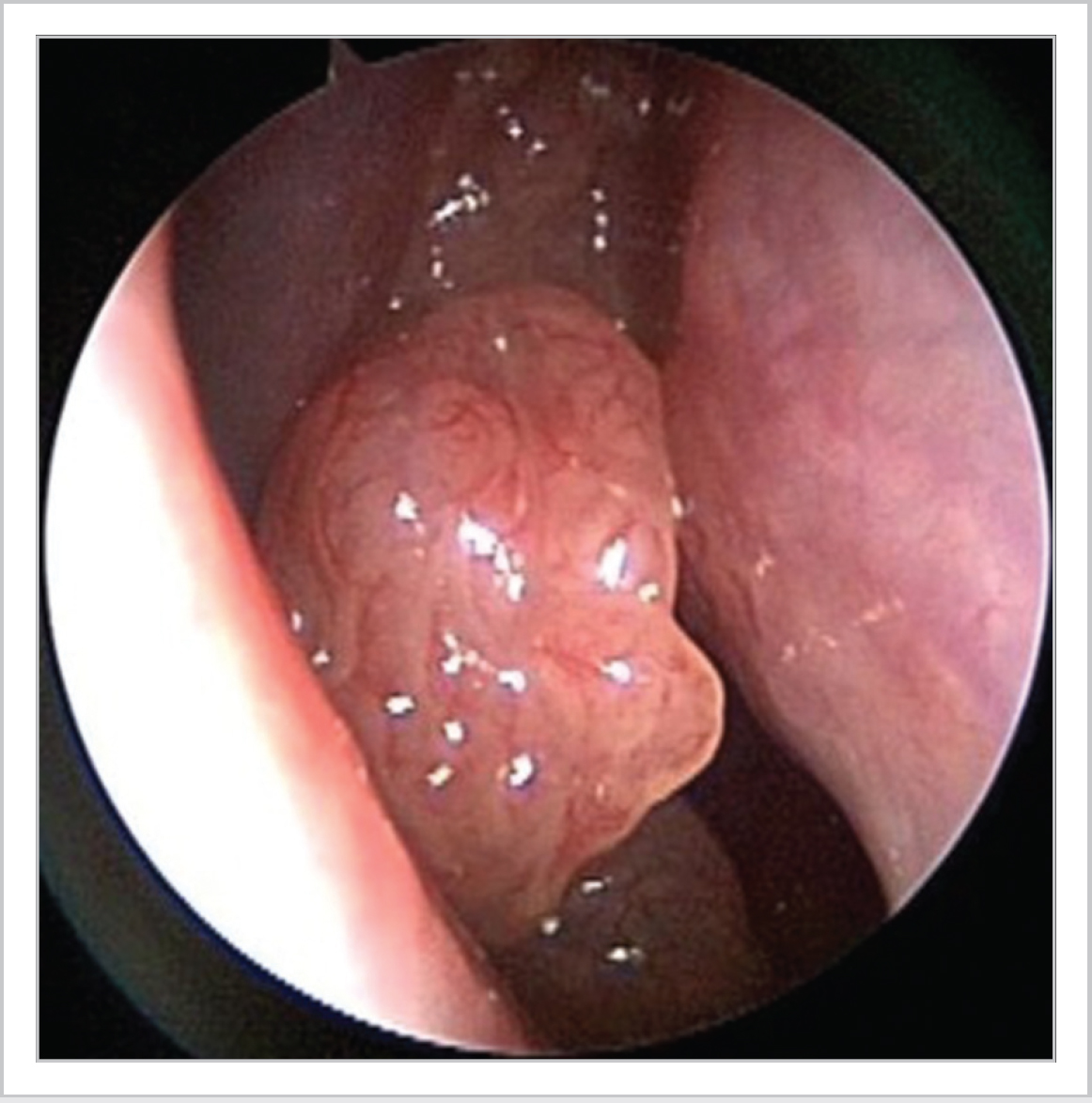
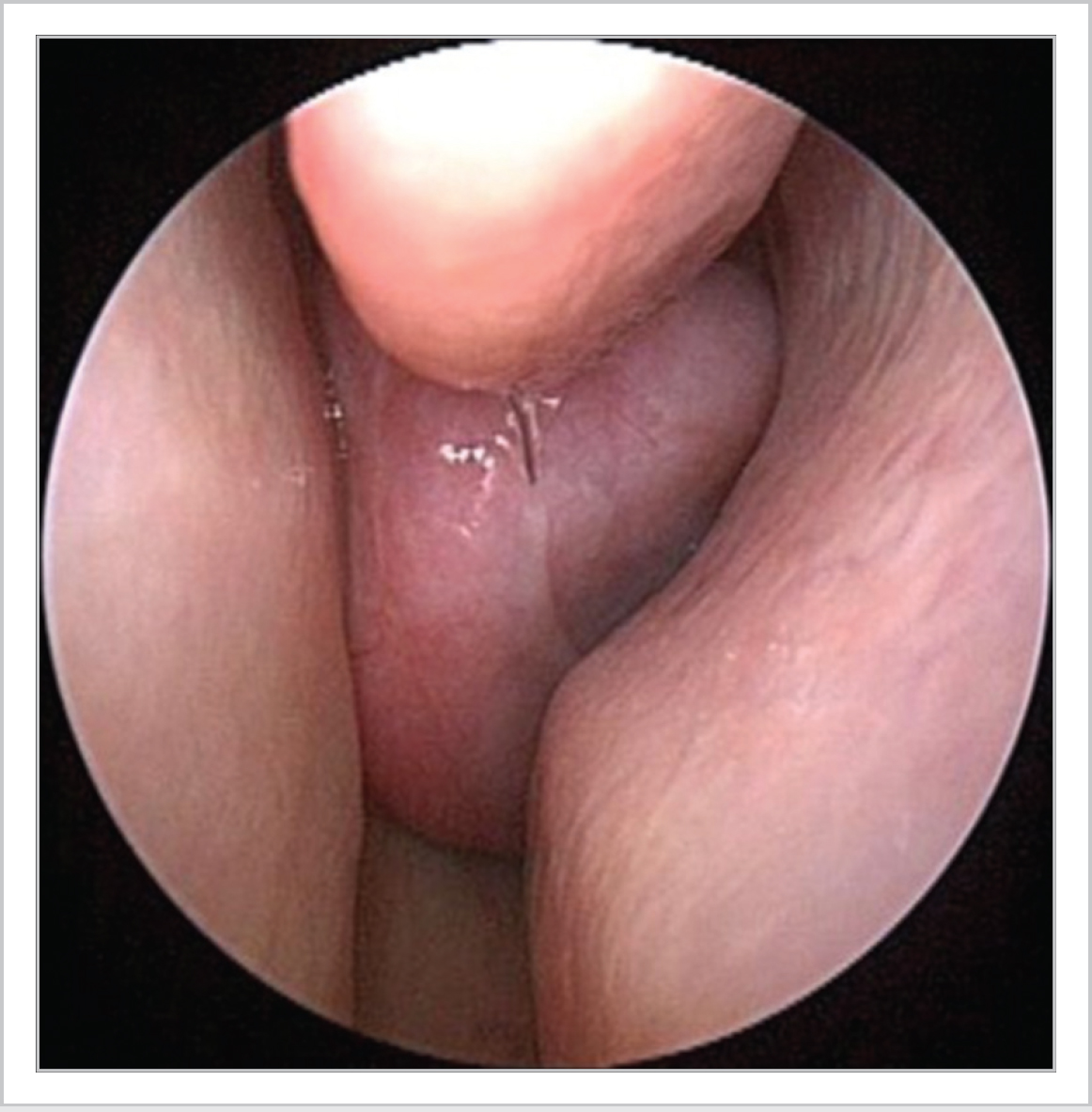
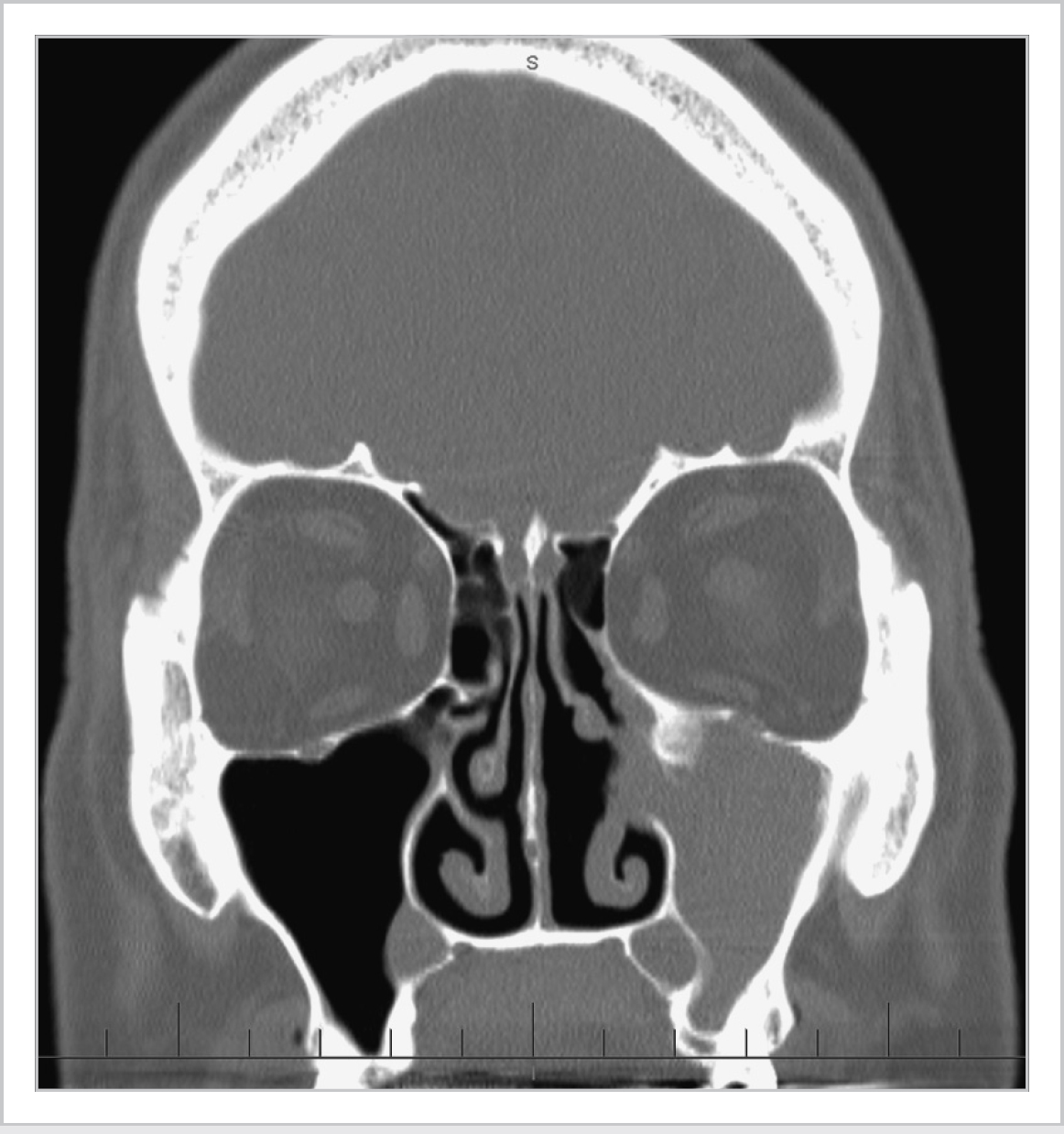
31 Tumours of the Nose and Paranasal Sinuses • Sinonasal neoplasms account for ~1% of all malignancies, 3 to 5% of head and neck (H&N) malignancies • 1/100,000/y incidence (UK/USA), M 2:1 F, 75% of malignant tumours in those >50 years • Hardwood dust (adenocarcinoma) • Toxin exposure (nickel, chromium, hydrocarbons, radium) • Snuff • Human papillomavirus (HPV) (cofactor) • Sinonasal tumours: • Sinus tumours: • Arise from nasal septum and nasal vestibule • Usually single • Associated with HPV types 6 and 11 • Most common benign sinonasal tumour (~1%), M2:1F, 2nd to 6th decade (mostly 5th–6th) • Frontal most common (57%), frontal lesions often silent and discovered incidentally • Ethmoid lesions may cause proptosis and usually invade the orbit • Gardner syndrome (AD)—multiple osteomas, soft-tissue tumours, and polyposis of colon • F>M, usually diagnosed in childhood (<20), 80% monostotic (1 bone involved) • Painless, swelling of maxilla or mandible, facial asymmetry ground glass appearance on CT • Ossifying fibroma = variant, peak age = 3rd to 4th decades, 75% mandible >~15% maxilla • 0.5 to 4% of all removed sinonasal tumours, ~1/1,000,000/y, M 2 to 5:1 F, peak 5th to 6th decade • Presents—unilateral polyp, epistaxis, rhinorrhoea, nasal obstruction, proptosis (Fig. 31.1) • CT—focal hyperostosis or osteitic changes indicate origin of lesion (Fig. 31.2) • Origin—maxillary (49%), frontal (18%), ethmoid (14%), sphenoid (12%), septum (5%), lateral wall (1%) (Table 31.1) • Histology—epithelium inverting into the stroma, intact basement membrane • Malignant transformation ~10%, treatment requires thorough removal of diseased mucosa • Endoscopic resection with medial maxillectomy (recurrence rate or rr: 12%) vs. open approaches (rr 20%) Fig. 31.1 Inverted papilloma. Fig. 31.3 Juvenile nasopharyngeal angiofibroma. • 0.5% of all H&N tumours, exclusively males, usually 7 to 19, rare >25, hormonal aetiology • Originates at sphenopalatine foramen, slow growing, locally invasive (Fig. 31.3) • Presents unilateral nasal obstruction (90%), epistaxis (50%), headache (25%) Table 31.1 Krouse staging system for inverting papilloma
31.1 Surgical Pathology
31.1.1 Epidemiology
31.1.2 Risk Factors
31.1.3 Site of Origin
 Nose 25%
Nose 25%
 Sinuses 75%
Sinuses 75%
 60 to 80% arise from maxillary sinus
60 to 80% arise from maxillary sinus
31.2 Benign Tumours
31.2.1 Exophytic Papilloma
31.2.2 Osteomas
31.2.3 Fibrous Dysplasia
31.2.4 Inverted (Transitional Cell) Papilloma
31.2.5 Juvenile Nasopharyngeal Angiofibroma
| I | Tumour confined to nasal cavity |
| II | Tumour involving osteomeatal complex and ethmoids and/or medial wall of maxillary sinus (with or without nasal cavity involvement) |
| III | Tumour involving any wall of maxillary sinus (but medial wall), sphenoid or frontal sinus, with or without stage II criteria |
| IV | Tumours with extranasal and extrasinus extension |
| Tumours associated with malignancy |
Table 31.2 Fisch classification system for JNA
| Stage | |
| I | Limited to nasal cavity, nasopharynx with no bony destruction |
| II | Invading pterygomaxillary fossa, paranasal sinuses with bony destruction |
| III | Invading infratemporal fossa, orbit, and/or parasellar region |
| IV | Invading cavernous sinus, optic chiasmal region, and/or pituitary fossa |
• Nasal mass (80%), orbital mass (15%), proptosis (10–15%)
• CT—extent of tumour, bowing of posterior maxillary wall
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


