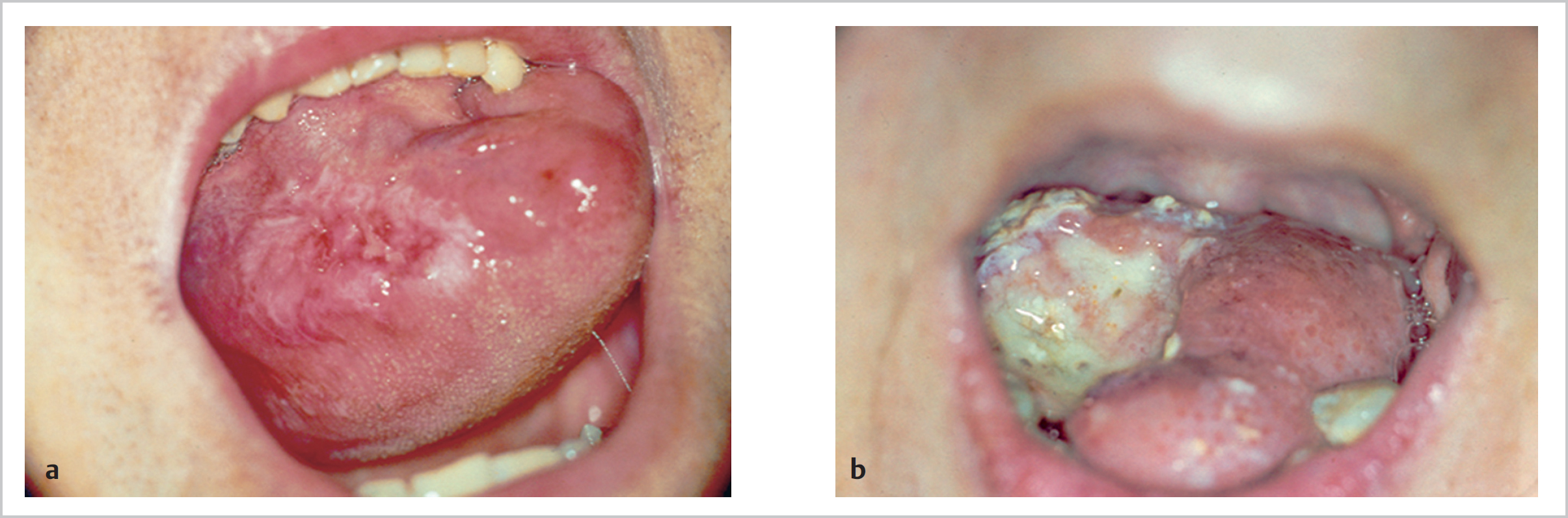
48 Tumours of the Lip and Oral Cavity • 6/1,000,000 • 93% lower lip, 5% upper, 2% angle • 2:1 male to female • 6th decade • White European ethnicity (×10) especially Celtic descent • Cigarette/pipe smoking • Poor dental hygiene • Chronic alcoholism (combined with smoking is 15× increased risk) • Chronic erosive skin diseases, e.g., lichen planus • Immunosuppression • Outdoor occupation • Squamous cell carcinoma (SCC) (98%) • Rare lesions • Upper lip and angular lesions metastasize sooner • <10% of lower lip lesions present with LN mets • T1—≤2 cm greatest dimension • T2—2 ≤4 cm • T3—>4 cm • T4a—invades adjacent structures e.g., cortical bone, inf. alveolar nerve, deep muscle of tongue, maxillary sinus, tooth socket (superficial erosion alone is insufficient) • T4b—invades masticator space, pterygoid plates, or skull base or encases the carotid a • Vermilion • Lower lip • Upper lip • Commissure • No sucking • Keep wound clean by removing crusts twice a day • Bactroban or fucidin may be applied • Half of external sutures may be removed at 3 to 4 days; rest removed at 1 week as appropriate • Soft diet • Abbe lip switch: • 300 kV orthovoltage X-ray therapy: 50 Gy in 15 fractions over 3 weeks • Interstitial therapy—rigid needles containing cesium • Variable worldwide incidence but accounts for 50% of all cancers in India • Male:female ratio 3–4:1 • More frequent after 5th decade of life • Buccal mucosa • Upper alveolus and gingiva • Lower alveolus and gingiva • Hard palate • Tongue—anterior 2/3 • Floor of mouth • Submucosa of inner surface of lips • Retromolar (parotid duct vicinity) • Mucous membrane of cheek • Floor of mouth • Lesser sublinguals (near major sublingual) • Glossopalatine (posterior to lesser sublinguals) • Palatine—hard and soft palate and uvula (not midline) • Lingual—inferior surface of tongue on each side of frenulum and at base and lateral borders of tongue • Small bony canals in hard palate • Greater and lesser palatine foramina • Lateral incisive foramina • SCC (85%) 3 types—exophytic, ulcerative, infiltrative • Malignant salivary (5%)—adenoid cystic, mucoepidermoid • Melanoma (1%) • Hodgkin lymphoma (0.1%) • Fibrosarcoma (0.5%) • Metastases to tongue—breast, lung, kidney most common • Tongue (lateral border; Fig. 48.1) (35%) • Floor of mouth (30%) • Lower alveolus (15%) • Upper alveolus (5%) • Buccal mucosa (10%) • Hard palate (3%) • Retromolar (2%) • Synchronous primary 10–15% larynx, oesophagus, lungs • Smoking-nitrosamines • High alcohol intake • Dental caries • Betel nut/tobacco chewing • Chronic glossitis • Malnutrition • Syphilis • Cirrhosis • Plummer–Vinson syndrome* • Lichen planus • Chronic hyperplastic candidiasis • HIV • Xeroderma pigmentosa • Congenital dyskeratosis • Submucosal fibrosis • Discoid lupus • Reverse smoking (Chutta, practiced in India) in hard palate cancer * Achlorhydria; iron deficiency anaemia; and mucosal atrophy of the mouth, pharynx, and oesophagus • Leukoplakia* (average ~5%) • Erythroplakia (75–90% show ca, ca in situ, or severe dysplasia) • Speckled leukoplakia (mixed white and red patches) increased risk of malignancy compared with leukoplakia alone * DDx-pemphigus, pemphigoid, lichen planus, candida, ill-fitting dentures, oral hairy leukoplakia • Incisional recommended • Biopsy red part if speckled leukoplakia • Staining with toluidine blue and Lugol’s iodine may help locate best biopsy site if multiple areas • Increased incidence of LN mets • Tumour can spread to tonsillar pillars, retromolar area, and floor of mouth • Large invasive carcinomas can extend beneath intact mucosa into muscles of posterior third of tongue and thence pre-epiglottic space • Tumour extends within musculature of tongue particularly in posterior direction beneath intact mucosa • Minor salivary gland malignancy (mucoepidermoid, adenoid cystic carcinoma) followed by SCC most common aetiology • Rarer pathology includes sarcoma, melanoma, or lymphoma • Presentation • See Table 48.1 • Site • Depth • Histology type
48.1 The Lip
48.1.1 Surgical Pathology
48.1.2 Risk Factors
48.1.3 Tumour Type
 Exophytic (commonest)
Exophytic (commonest)
 Verrucous
Verrucous
 Ulcerative
Ulcerative
 Melanoma
Melanoma
 Sarcoma
Sarcoma
 Salivary gland tumours (mucoepidermoid/adenoid cystic ca)
Salivary gland tumours (mucoepidermoid/adenoid cystic ca)
 Myoblastomas
Myoblastomas
 Pyogenic granulomas
Pyogenic granulomas
 Keratocanthoma
Keratocanthoma
 Granulomatous cheilitis, e.g., syphilis, sarcoid
Granulomatous cheilitis, e.g., syphilis, sarcoid
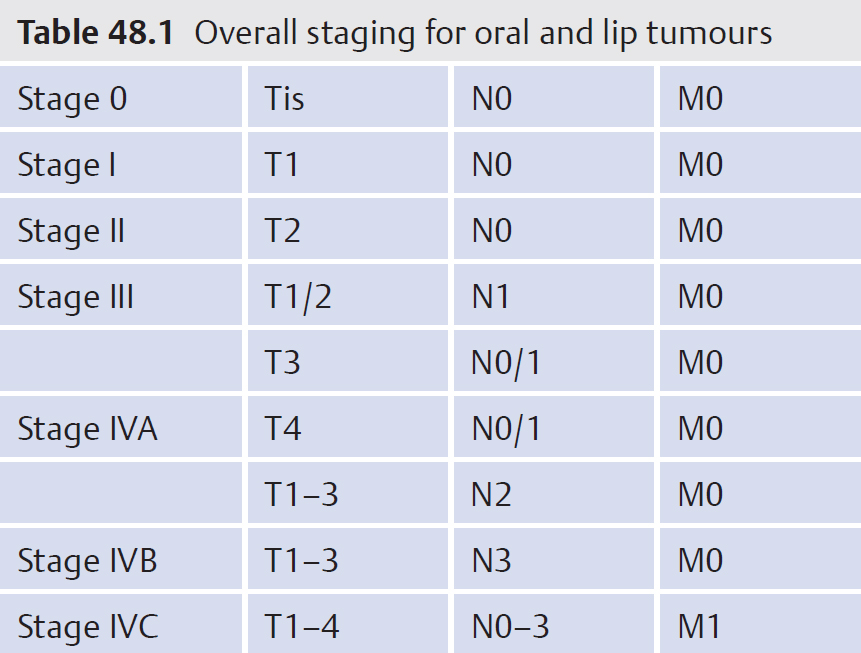
48.1.4 Staging
48.1.5 Repair of Defects
 Mucosal advancement
Mucosal advancement
 <1/3—primary closure
<1/3—primary closure
 1/3 to 2/3—Abbe*, Abbe Estlander, or Karapandzic flaps
1/3 to 2/3—Abbe*, Abbe Estlander, or Karapandzic flaps
 >2/3—bilateral Gillies fan flaps, axial scalp flap, or free tissue transfer
>2/3—bilateral Gillies fan flaps, axial scalp flap, or free tissue transfer
 <1/3—primary closure or Abbe flap
<1/3—primary closure or Abbe flap
 1/3 to 2/3—reverse Karapandzic or perialar advancement
1/3 to 2/3—reverse Karapandzic or perialar advancement
 >2/3—combination periala advancement or above techniques
>2/3—combination periala advancement or above techniques
 Abbe Estlander, double rhomboid flaps, or free tissue transfer
Abbe Estlander, double rhomboid flaps, or free tissue transfer
48.1.6 Aftercare following Lip Lesion Excision
 Feed patient with feeding cup or straw
Feed patient with feeding cup or straw
 Transect pedicle after 3 weeks as second stage and complete suturing
Transect pedicle after 3 weeks as second stage and complete suturing
48.1.7 Other Treatment Modalities
48.2 Oral Cavity
48.2.1 Anatomical Regions Subsites
 Mucosal surfaces of upper and lower lips
Mucosal surfaces of upper and lower lips
 Mucosal surfaces of cheeks
Mucosal surfaces of cheeks
 Retromolar areas
Retromolar areas
 Buccoalveolar sulci, upper and lower
Buccoalveolar sulci, upper and lower
Sites of Minor Salivary Glands
Channels of Spread of Tumours
48.2.2 Surgical Pathology Malignant Tumour Types
Sites of Squamous Carcinoma
Risk Factors
48.2.3 Premalignant Conditions
48.2.4 Biopsy Oral Lesions
Aggressive Features of Posterior Tongue Tumours
Hard Palate Tumours
 Swelling roof mouth
Swelling roof mouth
 Ill-fitting dentures
Ill-fitting dentures
 Nasal obstruction with extension into nose and maxillary sinus
Nasal obstruction with extension into nose and maxillary sinus
 Trismus with posterior extension involving pterygoids
Trismus with posterior extension involving pterygoids
 Middle ear effusion with extension into the nasopharynx, eustachian tube
Middle ear effusion with extension into the nasopharynx, eustachian tube
 Absent corneal reflex or palatal hypesthesia from invasion of maxillary division of trigeminal n in the sphenopalatine fossa
Absent corneal reflex or palatal hypesthesia from invasion of maxillary division of trigeminal n in the sphenopalatine fossa
 Masseter or temporalis wasting from invasion of mandibular division of trigeminal n
Masseter or temporalis wasting from invasion of mandibular division of trigeminal n
 Gingiva involvement with extension to upper or lower alveolus via dental sockets with loosening of teeth
Gingiva involvement with extension to upper or lower alveolus via dental sockets with loosening of teeth
 Lymph node involvement (levels I and II) in up to 30% of SCC ± retropharyngeal nodes
Lymph node involvement (levels I and II) in up to 30% of SCC ± retropharyngeal nodes
48.2.5 Overall Staging for Oral and Lip Tumours
48.2.6 Prognostic Factors
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


