(1)
Narayana Hridayalaya Multispeciality, Bangalore, India
Surgical Anatomy
Carcinoma of the tongue and floor of the mouth are one of the more aggressive oral cancers. The tumors have a tendency to spread locally as well to the lymph nodes and to the distant parts of the body. These characteristics make treatment of this tumor tricky. The tongue has a unique anatomy with muscle fibers crisscrossing allowing it to move in all directions. These muscles are broadly divided into intrinsic and extrinsic groups of muscles. This area is also rich in its vascular supply and lymphatic network and tumor has tendency to spread beyond local area at relatively earlier stages. The part near the midline has bilateral lymphatic drainage.
The tongue is broadly divided into the anterior tongue and base of the tongue which is rather considered as part of the oropharynx. The anterior 2/3rd is divided into two halves by median raphe. Lateral tongue mucosa continues beyond to floor of the mouth and to the alveolus (Fig. 8.1a). The mylohyoid muscle forms the infero-lateral diaphragm separating the sublingual gland from the submandibular gland. The genioglossus muscle attaches the tongue to the anterior mandible, while the hyoglossus muscle curves anteriorly to the hyoid (Fig. 8.1b). The entire unit is supplied by two lingual arteries entering through the hyoglossus muscle. The hypoglossal nerve provides the motor supply to the tongue running deep to the mylohyoid muscle entering the hyoglossus muscle.
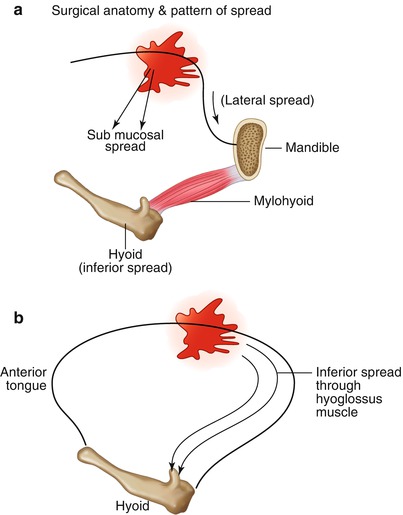
Fig. 8.1
Surgical anatomy and pattern of spread
Pattern of Spread
Tongue cancers are known for its aggressive and infiltrative nature and its submucosal spread. It is essential to palpate the induration around tumor before marking resection margin and a good habit is to continuously palpate the tumor while resecting. The lateral border of the tongue is mostly the first site to be involved, and then the tumor spreads laterally to the floor of the mouth and alveolar ridge (Fig. 8.1a). Mylohyoid insertion on the mandible usually limits its spread below and forms the basis for performing oblique marginal mandible resection. The deeply infiltrative tumor has the tendency to spread along hyoglossus muscle inferiorly, and this is the most common site for failure while performing intraoral tumor ablation (Figs. 8.1b and 8.2a).
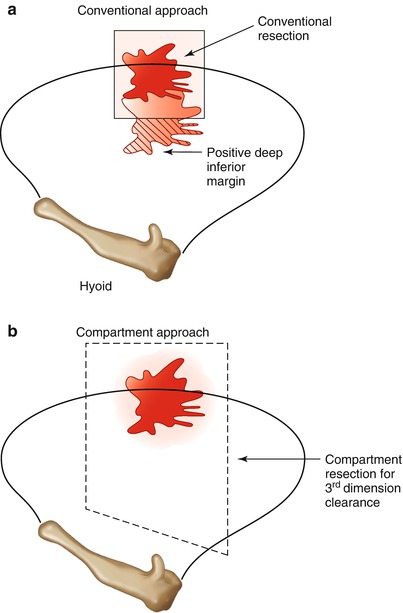
Fig. 8.2
Comparison between conventional and compartment (3D) surgical approach
The aggressive tumors also have tendency to spread across the midline though majority of lesions spread vertically. The inferior spread through the hyoglossus muscle is the most difficult area to address by conventional surgical approach. This forms the third dimension for infiltrative tongue or floor of mouth (FOM) tumors. Figure 8.2a, b proposes a concept for compartment tongue resection for deeply infiltrative lesions. The hyoglossus muscle is transected from its base, and thus the entire anatomical unit can be resected en bloc. This resection is also known as vertical resection compared to conventional horizontal resection. The chance of positive inferior margin is very rare.
Surgical Concepts
Figure 8.3 shows the algorithm for management of tongue cancers. Early T1 lesions can be managed by wide excision. The T2 lesion needs to be managed more aggressively with consideration for clearing deep margins. The larger T3 and T4 lesions need total glossectomy (TG) or near total glossectomy (NTG) preserving one side of the base of the tongue. More complex lesions can be managed by extended glossectomy along with mandible or larynx resection.
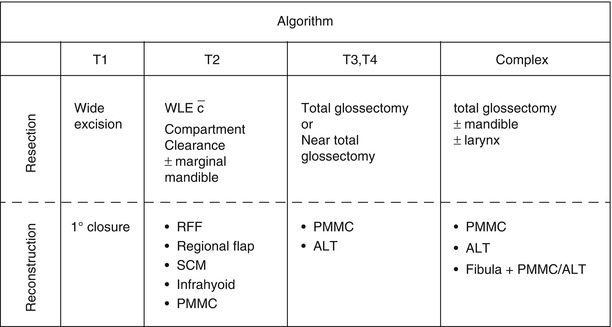
Fig. 8.3
Treatment algorithm for tongue and FOM cancer
Consider submucosal spread while planning resection margins.
Palpate the tumor all the time during surgery.
Infiltrative tumor has the tendency for inferior spread through hyoglossus, and removal of this muscle from hyoid is essential in achieving negative margins.
Ligation of lingual artery before primary resection significantly reduces bleeding during surgery.
Be aggressive on lymph node removal and consider bilateral removal for lesions crossing midline.
T1 Lesion
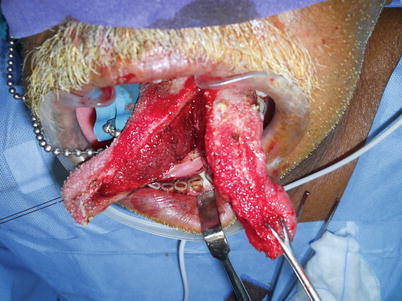
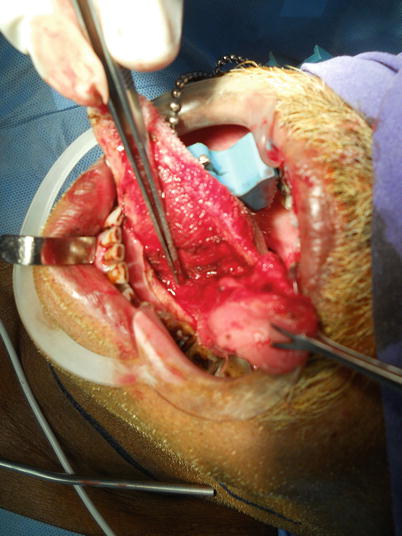
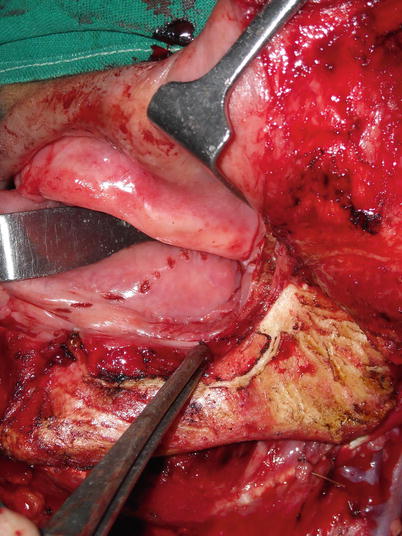
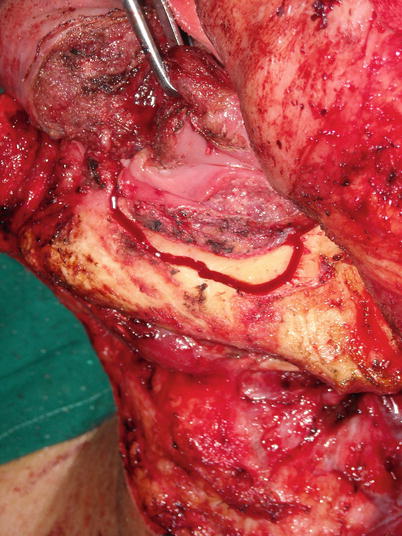
This section demonstrates surgical procedure for tongue and FOM cancers.















 < div class='tao-gold-member'>
< div class='tao-gold-member'>




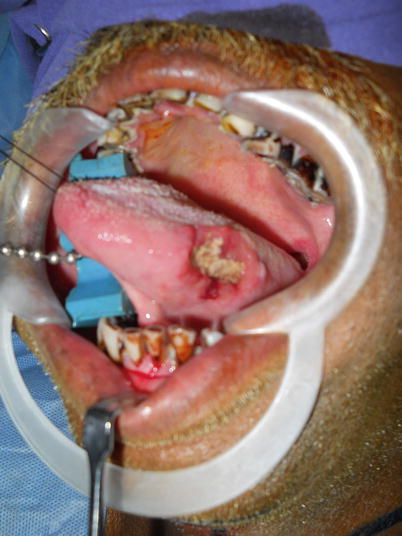
Fig. 8.4
Small primary lesion on lateral border of tongue
Fig. 8.5
Wide excision demonstrating 1.5 cm margin in all direction
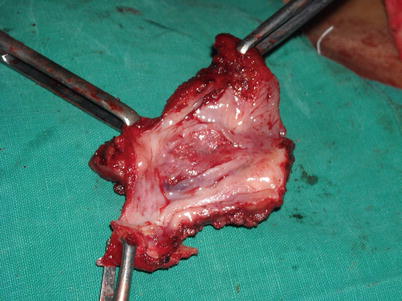
Fig. 8.6
Photograph showing specimen
Fig. 8.7
Primary closure of lesion. There is a great chance that these stitches will give way in postoperative phase. Alternatively one can leave this area raw to heal with secondary intention
Fig. 8.8
Photograph showing another lesion on lateral border of the tongue. This is an infiltrative lesion
Fig. 8.9
The inner marking is for induration. It is very important to palpate the induration and mark it. The 1–1.5 cm wide margin is removed from this marking and not from the visible ulcer margin
Fig. 8.10
Wide excision is performed
Fig. 8.11
The lingual artery is identified and ligated in depth
Fig. 8.12
Photograph shows complete resection superficially eroding mandible cortex with adequate hemostasis
Fig. 8.13
Reconstruction of the defect with lateral arm flap. This flap is ideal for such defect. Alternatively, one can use infrahyoid flap as local–regional flap for such defects
Fig. 8.14
The healed scar for lateral arm flap
Fig. 8.15
The anterior FOM lesion superficially eroding mandible cortex
Fig. 8.16
Proposed infrahyoid flap
Fig. 8.17
Flap insertion to reconstruct defect
Fig. 8.18
Healed flap
Fig. 8.19
The final outcome of this patient
Fig. 8.20
Healed scar for donor site. This flap is preferred over submental flap as donor site doesn’t involve any lymph node area
Fig. 8.21
Posterior FOM lesion abutting mandible
Fig. 8.22
Cheek flap is raised to have adequate exposure
Fig. 8.23
Marginal mandibular resection
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
