(1)
Narayana Hridayalaya Multispeciality, Bangalore, India
Surgical Anatomy and Pathology
Parotid gland surgery is interesting because the facial nerve traverses through its substance. The entire procedure revolves around removing the tumor while preserving branches of the facial nerve. Figure 4.1 shows the schematic anatomy of the facial nerve. The nerve comes out of the stylomastoid tunnel and enters the gland. It can be identified anterior to posterior most fibers of digastric muscle that is inserted on mastoid. Identification of the tragal pointer and digastric tendon serves as a guide to facial nerve. The nerve divides into two main trunks which further divide into five branches. These branches run through the gland and become more and more superficial in the periphery. The terminal parts of the branches run deep to the buccinator muscle in the subcutaneous plane. The braches to eye and angle of mouth are most important in terms of functions.
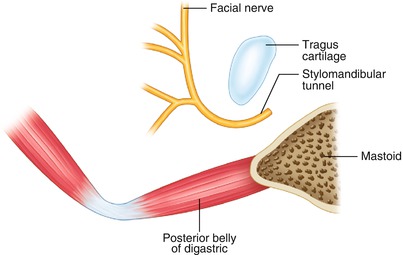
Fig. 4.1
Schematic representation of facial nerve anatomy
The parotid neoplasm can be classified as benign and malignant lesions (Fig. 4.2). The malignant ones are further subdivided into low-, intermediate-, and high-grade lesions. The surgical extent remains the same for all these lesions, and the aim is to remove the entire lesion with cuff of normal tissue all around. If nerve function is normal in the preoperative phase, it is possible to preserve it in the postoperative phase in majority of cases. Salivary gland pathology is complex, and it is not always feasible to establish exact diagnosis before surgery. The fine-needle cytology is advisable in every case, and this can be helpful in counseling of the patient regarding management of the facial nerve. The operative procedure remains unchanged irrespective of pathology.
Fig. 4.2
Treatment algorithm
Surgical Concepts
Removal of lesion with cuff of normal tissue around is called adequate parotidectomy and is current standard of care for parotid neoplasm. This is performed irrespective of pathology.
The margin on the nerve is often positive in the pathology report, and it is not possible to have cuff of normal tissue on this margin. If the capsule of the tumor is intact, this is considered negative margin, and intraoperative decision by the surgeon is considered adequate in deciding adjuvant treatment.
In the case of nerve involvement, the nerve must be sacrificed. It is not advisable to leave behind gross residual disease on the nerve. One can consider leaving behind microscopic disease in some low-grade malignancies.
The nerve must be repaired by interposition nerve graft if resected.
Neck dissection is performed for node-positive lesions only. Some surgeons advocate performing selective neck dissection for high-grade neoplasm. Some surgeons also advocate frozen section of sampled lymph node in level II area.
Radiotherapy is reserved for high-grade neoplasm, neck node-positive case, large lesions (T3 and T4), and recurrent malignant neoplasm.
An inappropriately operated parotid case poses a difficult challenge. Re-exploration is considered only if there is reasonable doubt about previous surgery, biopsy suggests grossly inadequate previous surgery, and imaging studies reveal residual lesion.
Superficial Lobe Parotid Lesion
This procedure demonstrates adequate parotidectomy for superficial lobe parotid tumor.


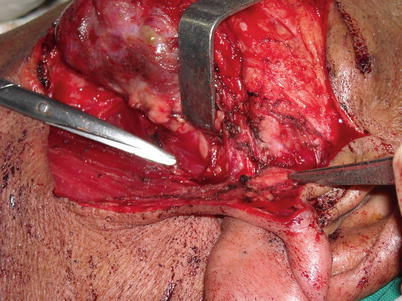
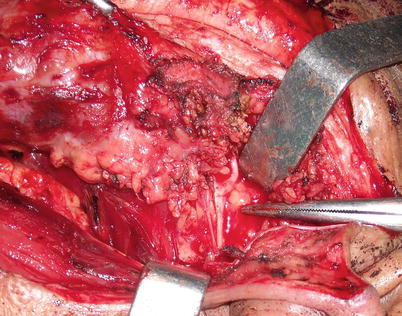
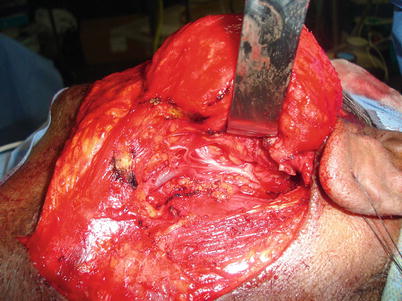
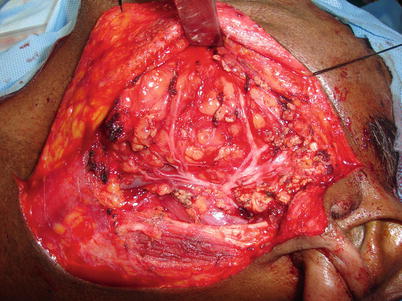
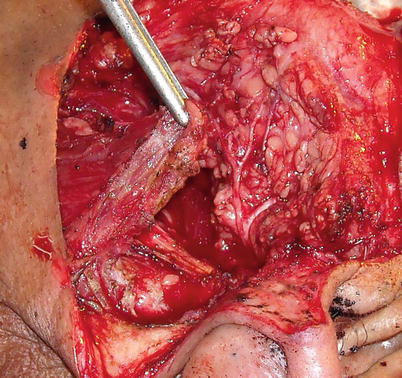



Fig. 4.3
Patient with parotid swelling. The incision is marked in “s” shape. It is important to have a gentle wide curve for the postauricular part to avoid tip necrosis
Fig. 4.4
Flap is raised in subcutaneous plane. Branches of fascial nerve become superficial in periphery and hence this area should be carefully dissected
Fig. 4.5
The photograph shows posterior belly of digastric muscle and tragus cartilage. Nerve can be located in the middle of these two landmarks. There is always a small vessel just superficial to the nerve, and this can be considered as an important guide to the facial nerve
Fig. 4.6
The nerve is identified. It is mandatory to identify its bifurcation before labeling it as the facial nerve
Fig. 4.7
The lesion is slowly mobilized preserving all branches of the nerve
Fig. 4.8
Complete tumor removal with preserved branches of the facial nerve
Fig. 4.9
The anterior portion of the sternocleidomastoid (SCM) can be used as local rotation flap to improve the aesthesis
Fig. 4.10
Flap is sutured to the remaining gland
Fig. 4.11
Final outcome
Fig. 4.12
Photograph showing side view demonstrating utility of SCM flap
Deep Lobe Tumor
This procedure demonstrates removal of the deep lobe parotid tumor.



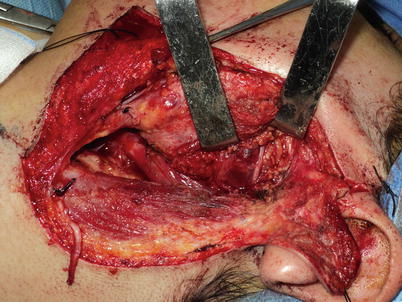





Fig. 4.13
Incision for parotidectomy
Fig. 4.14
Flap being raised
Fig. 4.15
Exposed posterior belly of the digastric muscle
Fig. 4.16
Identification of the facial nerve trunk. The tumor is pushing the nerve anteriorly
Fig. 4.17
In the case of recurrent parotid lesions where it is difficult to identify main trunk due to fibrosis, identification of peripheral branches of facial nerve serves as a good guide in tracing main trunk
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
