(1)
Narayana Hridayalaya Multispeciality, Bangalore, India
Surgical Anatomy and Pathology
The parapharyngeal space is an imaginary space situated lateral to the pharyngeal tube containing vital neurovascular bundles. It is an inverse triangle where the base is formed by base of skull, while apex is formed by hyoid bone. This space is strategically situated in the head and neck as tumor starting from the pharyngeal mucosa spreads laterally and this space proves as a barrier to deep spread. Isolation of the tumor base early in this space makes clearance easy and complete at depth. Figure 6.1 demonstrates the important neurovascular bundles that traverse this space. It essentially contains the carotid artery and branches of external carotid artery and internal jugular vein. Various cranial nerves run along and across this space. Ligation of branches of the external carotid artery and parapharyngeal venous plexus exposes the parapharyngeal space.
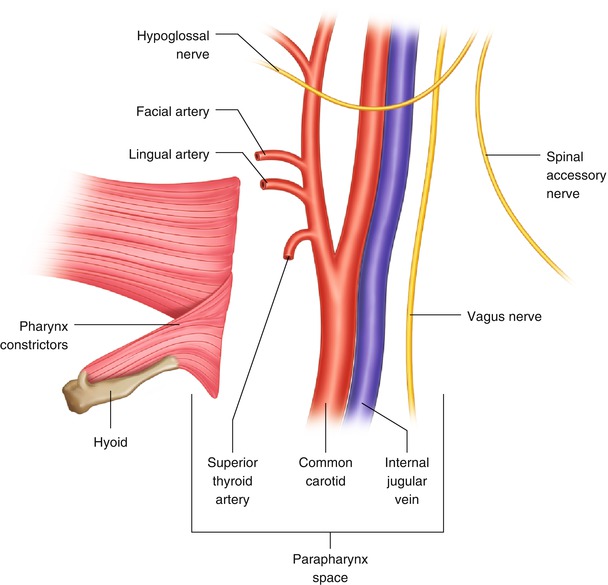
Fig. 6.1
Schematic representation of surgical anatomy
Figure 6.2 demonstrates cross-sectional anatomy of the parapharyngeal space. The band connecting the styloid process and pterygoid plate divides this space into an anterior pre-styloid compartment and a posterior post-styloid compartment. The pre-styloid space contains the deep lobe of the parotid, minor salivary gland, parapharyngeal fat pad, and few lymph nodes. The post-styloid compartment contains the carotid sheath and cervical sympathetic chain. The diagnosis of tumor in this space is essentially made by understanding the anatomy of this space. Imaging study with a CT scan or magnetic resonance imaging (MRI) classifies the lesion as a pre-styloid or post-styloid one. This provides a differential diagnosis regarding the origin of the tumor. The tumor arising from the pre-styloid compartment generally presents as an intraoral bulge and displaces the parapharyngeal fat pad posteriorly, while the post-styloid tumor presents as a lump in the neck and pushes fat anteriorly. The carotid sheath is pushed posteriorly by the pre-styloid tumor, and the stylomandibular tunnel is widened in case of deep lobe parotid lesion. For long-standing pre-styloid lesions, the posterolateral wall of the maxilla can be pushed anteriorly due to persistent pressure. The post-styloid lesions generally arise from the carotid sheath, and the carotid body tumor is one of the most common among them. This tumor originates from the carotid bulb area and splays both carotid arteries that can be clearly demonstrated in scans. The nerve sheath tumors arising from the vagus and sympathetic chain are located posterior to the carotid vessels. It is essential to remember that tissue diagnosis is not routinely required in parapharyngeal space lesions. Imaging is a primary diagnostic modality and diagnosis is based on its location and understanding of the anatomy. Fine-needle cytology (FNAC) should always be considered after confirming findings of imaging study to avoid injuring vascular lesions.
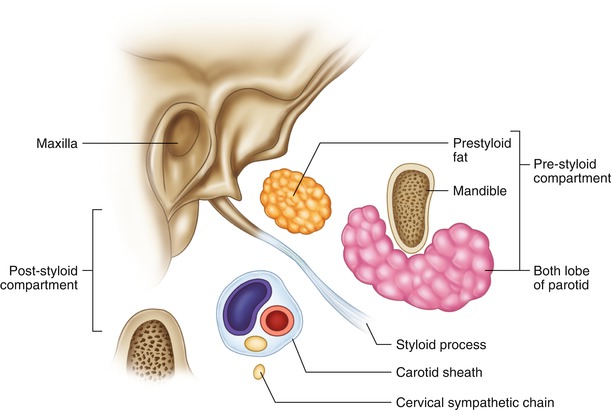
Fig. 6.2
Classification of parapharynx space
Surgical Concepts
Diagnosis is based on imaging study. Understanding of surgical anatomy is key in identifying the origin of the lesion.
The concept is to identify all nerves and vessels early in the surgical procedure rather than trying to focus on removing the tumor. This enables us to avoid injury to any important structure, and in the process the tumor automatically gets mobilized.
The pre-styloid lesions generally originate from deep lobe of the parotid or minor salivary gland, and transcervical or trans-parotid surgical approaches are commonly preferred.
The post-styloid tumors are generally approached from the transcervical route (Fig. 6.3). The conventional mandibulotomy approach for high parapharyngeal space lesions is almost obsolete in the current surgical practice. The vast majority of lesions can be removed through the neck by mobilizing the mandible anteriorly by releasing the stylomandibular ligament. Ligation of external carotid artery can expose high parapharyngeal space, and these lesions can be easily addressed.
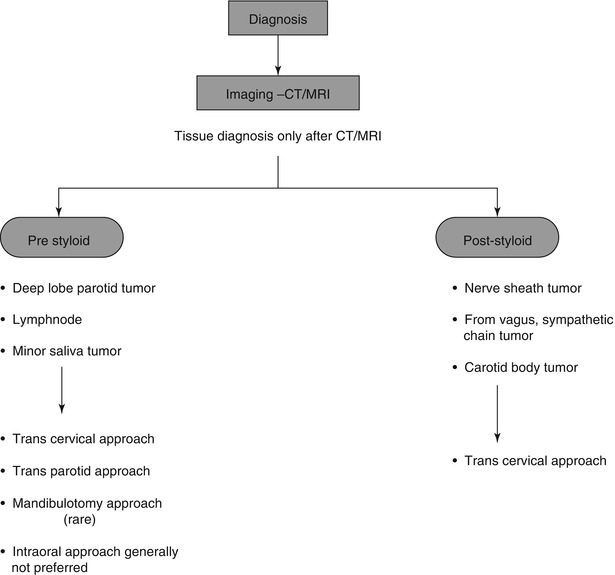
Fig. 6.3
Treatment algorithm
It is advisable to pack this space with absorbable hemostatic materials to prevent persistent postoperative bleeding.
Post-styloid Tumor
This procedure demonstrates removal of a nerve sheath lesion arising from the cervical sympathetic chain in post-styloid space.


 < div class='tao-gold-member'>
< div class='tao-gold-member'>




Fig. 6.4
Presentation of a patient with deep upper cervical swelling. The pre-styloid lesion generally presents with an intraoral swelling
Fig. 6.5
Surface marking of cranial nerves – vagus, spinal accessory, and hypoglossal nerves
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
