(1)
Narayana Hridayalaya Multispeciality, Bangalore, India
Surgical Anatomy
The buccal mucosa complex essentially consists of the buccal mucosa (BM), gingivo-buccal sulcus (GBS), lower alveolus, and retromolar trigone (RMT). The buccal complex consists of four layers starting with the mucosa, buccinator muscle, subcutaneous tissue, and skin (in to out). The branches of the facial nerve run in subcutaneous tissue planes over the buccinator muscle. The average distance from mucosa to skin is approximately 1–1.5 cm, and it is very easy for infiltrating tumors to travel across and involve the outermost level. The GBS is located at the junction of the buccal mucosa reflecting over the alveolus. The cancer occurring at this site is very common in the Indian subcontinent due to the habit of tobacco chewing. The retromolar trigone has a unique anatomy with potential for tumor spread into the masticator space. The RMT is bounded below and above by the alveolar ridge, medially by the tonsil, and laterally by the buccal mucosa. It is the third dimension – the base that holds the key to the tumor spread. The mucosa lies directly on ascending ramus of the mandible. The masseter muscle lies lateral to the mandible, and the medial pterygoid muscle lies medial to the mandible with lingual and inferior alveolar nerve running through its substance. The temporalis muscle gets inserted on the coronoid process, and the lateral pterygoid muscle occupies the top half of the masticator space.
Surgical Pathology and Pattern of Infiltration
This complex can be divided into anterior region and posterior region for understanding the pattern of infiltration and planning the surgical approach. The anteriorly located tumors spread laterally to involve soft tissue and skin while posteriorly located tumors spread through the RMT to masticator space (Figs. 7.1, 7.2, and 7.3). The surgical approach remains distinctively separate for both groups of tumors.
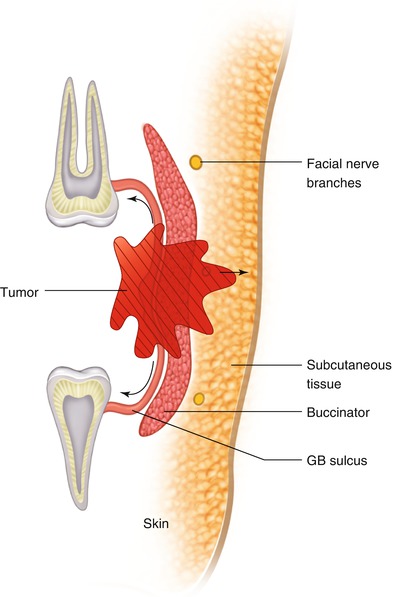
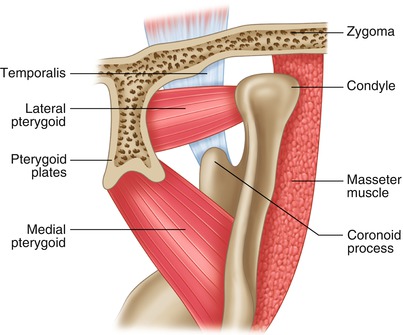
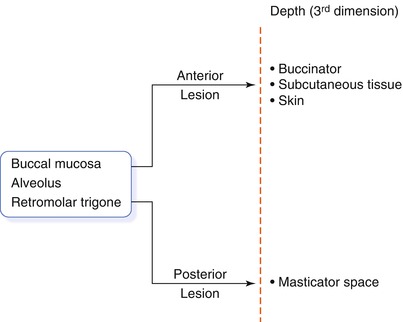
Fig. 7.1
Surgical anatomy and tumor spread in anterior compartment
Fig. 7.2
Anatomy of masticator space and tumor spread in posterior compartment
Fig. 7.3
Conceptual diagram for proposed 3-D resection
The anteriorly located infiltrative tumors have a tendency to invade through the layers of buccal mucosa and fungate through the skin. These tumors start from mucosa and easily infiltrate the buccinator muscle. Involvement of the subcutaneous tissue is also not uncommon and seen quite early in the disease progress. It is strongly recommended to remove one layer extra to get negative margins at depth. The skin invasion is considered a sign of aggressive biology in conventional thinking, and many patients are offered only palliation. This infiltration of the skin is just due to the close proximity to the mucosa and a natural progression of disease. If adequately resected, outcome of these patients have been comparable to other advanced lesions in our experience. The GBS tumors show paramandibular spread mainly due to their location (Fig. 7.4). The actual invasion of the mandible is seen in very few cases even with large soft tissue involvement. It is technically feasible and oncologically safe to perform marginal mandibular resection if bone is not involved – the soft tissue margins need to be adequate. The alveolar tumors generally infiltrate the mandible and then spread either towards the lingual or buccal side.
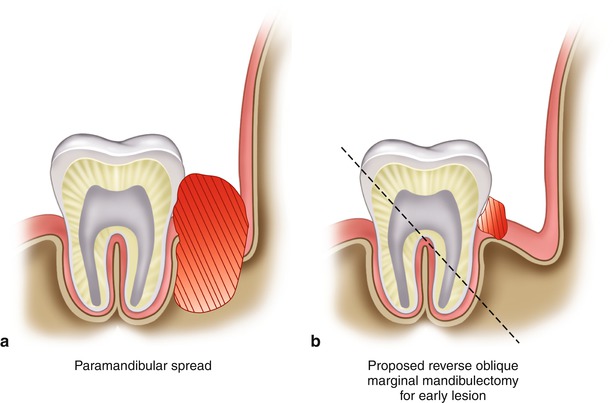
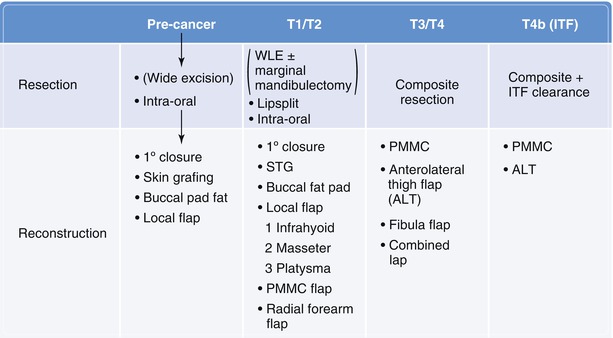
Fig. 7.4
Gingivo-buccal sulcus tumor ÷ pattern of spread
Fig. 7.5
Treatment algorithm
The posteriorly located lesions tend to infiltrate masticator space (Fig. 7.2). The early lesions of RMT have the potential to invade the mandible, masseter, and the medial pterygoid muscle. It is essential to evaluate the involvement of these structures before planning any conservative surgery. The gross infiltration of masticator space warrants complete clearance of soft tissue in infratemporal fossa. Involvement of lateral pterygoid muscle and pterygoid plate is no longer considered contraindication for surgery. The spread of tumor to pterygomaxillary tissue is considered a relative contraindication as chance of intracranial tumor spread is relatively high.
The buccal cancer patient with history of tobacco chewing commonly presents with premalignant changes in surrounding mucosa and submucous fibrosis. These two factors have significant bearing on surgical planning. It is essential to try and include the area of premalignancy into surgical resection margin. The submucous fibrosis causes trismus that reduces the mouth opening and influences the resection approach and reconstructive options.
Surgical Concepts
Anteriorly located, superficial lesion with adequate mouth opening can be resected through the intraoral approach. It is essential to include buccinator muscle in resection for any malignant lesion.
Posteriorly located tumors are better approached through lip-split incision.
It is acceptable to perform marginal mandibulectomy for early GBS cancer abutting but not invading mandible. This is particularly useful for anteriorly located lesions and for patients with minimal submucous fibrosis.
It is advisable to perform segmental mandibular resection for more advanced lesions with paramandibular spread.
The posteriorly located tumors with moderate to severe submucous fibrosis do better with segmental resection compared with marginal resection in terms of functional outcome.
Tumors in the RMT region are tricky to resect, and it is better to be aggressive with these lesions. The local recurrences at skull base after conservative approach are very common and difficult to salvage.
Precancer Lesions
Approach: These lesions can be excised by intraoral approach in majority of cases. the lip split approach may be required for extensive lesions with associated fibrosis.



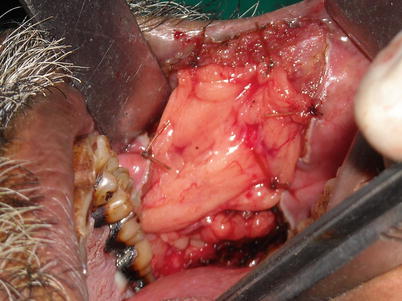

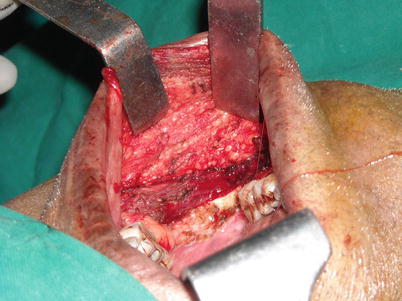

Fig. 7.6
This is a premalignant lesion involving angle of mouth and anterior buccal mucosa. It is important to include all unhealthy mucosa in resection margin. This becomes a bit difficult in certain cases where mucosa of the entire oral cavity is unhealthy, but at least the premalignant lesion needs to be resected
Fig. 7.7
The photograph showing extent of resection. It is better to include buccinator muscle in your resection base if lesion is a malignant one. It is sufficient to remove the mucosa and submucosa and superficial part of the buccinator muscle for purely premalignant lesion
Fig. 7.8
Postoperative recovery after 1 week of surgery. Repair of angle of mouth and approximation of lip muscles are key in maintaining continence
Fig. 7.9
Similar defect being repaired by buccal pad of fat. The fat pad is situated in the infratemporal fossa region and can be easily teased out to repair small buccal defects
Fig. 7.10
Result after 10 days of healing
Fig. 7.11
Removal of entire buccal mucosa and buccinator muscle for extensive precancer lesion
Fig. 7.12
Reconstruction with split thickness skin graft (STG). It is essential to fix the graft with bolster in cheek with through and through stitch. In majority of cases, STG gradually comes off but acts as biological dressing and improves mucolization. Trismus is a real problem with this kind of reconstruction, and it is essential to do rigorous mouth opening exercise for a period of 6–12 months
T1–T2 Lesions
Approach: Intraoral if small lesion with adequate mouth opening. Lip-split approach is preferred for large, infiltrative, or posteriorly located tumors and with associated trismus.
Intraoral Resection
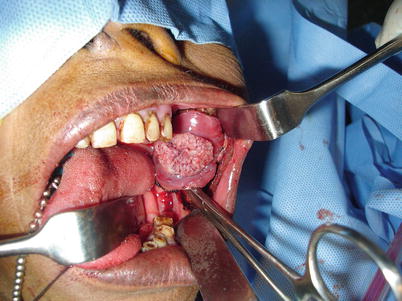
Fig. 7.13
A verrucous lesion of anterior buccal mucosa. These lesions are more exophytic than infiltrative and can be ideally approached without lip split

Fig. 7.14
It is advisable to include buccinator muscle in base. The branches of facial artery run across the field and securing them early in resection (below and posterior aspect) reduces bleeding. The branches of facial nerve run deep to the buccinator in subcutaneous tissue. These branches can be preserved for superficial lesions by keeping some fibers of buccinator muscle. It is our strong recommendation not to compromise on resection at depth in case of infiltrative lesion to preserve facial nerve branches

Fig. 7.15
Photograph showing ligated branches of facial artery. The subcutaneous tissue is visible in bed demonstrating removal of buccinator muscle in specimen

Fig. 7.16
The infrahyoid local flap being inserted for defect

Fig. 7.17
Flap in position

Fig. 7.18
Photograph after 1 month of procedure

Fig. 7.19
Infiltrative lesion in anterior buccal mucosa with no trismus

Fig. 7.20
The way to feel for involvement of subcutaneous tissue or skin

Fig. 7.21
The planning included part of the skin even though it was not obviously involved. It gives complete control of removal of base, and there is no chance of positive margin at depth
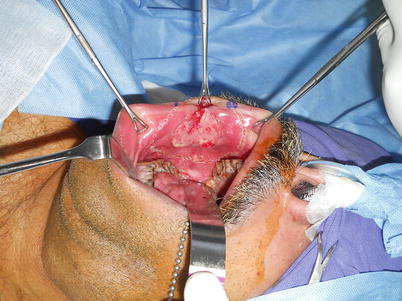
Fig. 7.22
Mucosal markings with adequate margins

Fig. 7.23
Resection including skin

Fig. 7.24
Planned primary closure with buccal pad of fat for cover

Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


