Tumors Metastatic to the Orbit in Adults
Ira Vidor
Jennifer A. Sivak-Callcott
Jeffrey Hogg
H. James Williams
Definition, Prevalence, Etiology
This chapter discusses lesions that spread to the orbit from noncontiguous sites, which is more common in adults. Lymphoproliferative/leukemic disease is presented in Chapter 39. Childhood metastatic orbital masses are included in Chapter 27.
Diagnosis of metastatic orbit disease has been a challenge since its first report by Horner in 1864.1 The diverse nature of primary tumors results in a wide breadth of clinical presentation. Historically, orbital metastasis portended a poor prognosis for survival, but the modern era of medicine has brought new advances in cancer therapy. These achievements have reduced morbidity and dramatically increased life expectancy.
Most cancers that spread to the orbit in adults are carcinomas.2,3,4 The most common metastases vary by geographic region. In North America and Europe, breast cancer is the most frequent orbital metastasis, accounting for 27% to 59% of cases. It is followed by lung, prostate, melanoma, and renal cell carcinoma.2,5,6,7,8 In Japan, lung cancer is most common followed by breast, liver, and stomach cancer9 (Table 45.1). These differences may represent the overall incidence of the primary tumors in these parts of the world.
Table 45.1 Tumor Types by Review | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Over the last century, the numbers of cancer cases and reports of orbital metastases have increased.3,7,8 In 1944, Godtfredsen10 reported that ocular metastasis occurred in only 0.7% of tumors. The 1967 article of Albert et al11 found 4.7% of cases with metastatic disease had orbital or ocular metastases. Increased reporting, improved clinical surveillance, more advanced diagnostic techniques, and longer survival may account for this increase. Despite contemporary medical advances, some orbital metastases are not discovered until autopsy. Dreing et al12 found 10% to 30% of breast cancer patients had clinically silent orbital lesions, and Bloch and Gartner13 found histopathologic evidence of ocular or orbital metastasis in 12% of patients.
Metastatic lesions account for 1.5% to 8% of orbital disease.4,14,15,16,17,18,19,20,21 In patients older than 60 years of age, this percentage is higher (10%).2 There is a discrepancy as to male:female predominance, although most reviews report a female majority up to 76%.6 This inconsistency may be owing to regional differences in type of primary tumor, as reports from Japan state that 59% of patients are male, but the incidence of breast cancer is lower in Japan than in the United States.22
Although most patients with orbital metastasis have a history of cancer, as many as 19% to 42% present to the ophthalmologist without a known primary tumor.2,5,6,7 The ophthalmologist should maintain a high index of suspicion for metastatic lesions when evaluating orbital disease and specifically inquire about cancer in the medical history. This is of increased importance when assessing elderly patients.23
The process of metastasis is fascinating, and many ideas have been proposed. In 1889, Stephen Paget24 published his concept of organ specific metastasis, which is a subject of modern research.25 In 1928, James Ewing (26) set forth his mechanical hypothesis whereby blood flow route determined pattern of spread. Historically, authors have contended that tumors had a predilection for the left orbit.27,28,29 This supported Ewing’s theory, as blood flow from the heart is more direct to the left orbit because the left common carotid artery branches off the aorta whereas the right arises from the brachiocephalic artery.30 Recent papers contest this, showing both orbits to be equally affected.2,7,28,29,30,31,32
Modern theory of metastasis consists of five parts: The primary cancer attracts vascular ingrowth; tumor cells break away, invade the vascular or lymphatic systems, and survive; these tumor cells lodge in postcapillary venules of the targeted organ; they then pass across the venule wall into tissue parenchyma and grow.33 A malignant cell’s ability to metastasize depends on how well it interacts with adhesion molecules and how well it forms adhesive bonds with tissues at each of these steps.33 The metastatic process can be thwarted by the body’s immune system at any of these points.
In 1997, Hartstein et al33 described integrins and studied them in orbital metastatic disease. Integrins are a family of dimer receptors that act as adhesion molecules on tumors cells, facilitating cell to cell and cell to extracellular matrix interaction. Integrin expression changes when a cell undergoes malignant transformation. Hartstein et al studied tissue from four orbital biopsies. They found increased integrin subunit expression in 2 cases of metastatic prostate cancer (beta 3 expression) and 1 case of metastatic cutaneous melanoma (beta 3, alpha 2 and alpha 4). One case of breast cancer proved equivocal.33 Contemporary research continues to define the mechanism by which metastasis takes place.
Traditionally, metastases to the orbit were considered solely a hematogenous process since the orbit was thought to be devoid of lymphatics.34 Recently, enzyme histochemistry has identified lymphatics in the lacrimal gland and dura of the optic nerve. In addition, structures demonstrating positive staining for markers highly suggestive of lymphatics have been found in the orbital apex.35,36 This suggests the possibility that orbital metastasis occurs via hematogenous or lymphatic routes.
Clinical Features
Temporal onset, clinical signs and symptoms, treatment, and outcome of metastatic orbital disease are largely a function of the primary tumor. In general, orbital symptoms are present 3.6 months before ophthalmologic evaluation.7 Lung metastases manifest quickly and patients have been treated for an inflammatory process,4 whereas breast and thyroid cancer tend to have a longer duration of symptoms.4,7 Overall, orbital metastases have a more rapid onset than other types of orbital neoplasia.
The average time between primary tumor diagnosis and orbital metastasis varies with each cancer type.2,7 Overall, the time from initial diagnosis to orbital metastasis ranges from 31 to 71 months. Breast cancer averages 4.5 to 6.5 years before orbital metastasis, but has been documented up to 27 years later.4,37 In thyroid cancer the average time is 5 years. Lung cancer has a more acute onset at an average of 1.4 months.7,8
Although a known primary tumor is common in breast and cutaneous melanoma metastases, this is not the case in other malignancies. In up to 87.5% of lung carcinoma orbital metastases, the orbital lesion is the initial presentation of cancer.7,9 As few as 16.4% of patients with renal cell metastases have a known primary cancer.38
Limited ocular motility and diplopia are the most common presenting sign and symptom of orbital metastasis (48%–63% of patients). This is followed closely by proptosis (26%–68% of patients) (Table 45.2). The amount of decrease in motility is often greater than expected for the degree of globe displacement. Other common presenting abnormalities include ptosis (32%–49%), mass (15%–61%), decreased vision (9%–43%), pain (3%–20%), and enophthalmos (8%–22%).2,4,5,6,7,39,40 If pain is present, the clinician should be highly suspicious for metastatic disease as this is usually an initial manifestation. Pain is often nagging in character and may indicate an apical lesion or metastasis to bone.4 Rare symptoms include paresthesias, pulsation, disc edema, and subconjunctival hemorrhage.4,7,9 Enophthalmos is present in 8% to 10% of cases, most of which are caused by breast carcinoma. Enophthalmos occurs by one of two mechanisms, contraction of soft tissues or bony loss, “physiologic decompression.” This finding can be easily missed if not specifically examined. Pulsation of the orbit in metastatic disease has been described and also occurs by one of two mechanisms: destructive bone loss that allows transmission of cerebral spinal fluid pulsation, and high internal blood flow within the metastasis. This latter mechanism can be seen in renal and thyroid cancer.4,7,40,41,42,43,44,45
Table 45.2 Presenting Sign or Symptom in Patients with Orbital Metastasis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Orbital metastasis can occur in any anatomic position. Shields et al2 determined that 41% of metastases were located in the anterior orbit (eyelids to posterior sclera) and 27% in the posterior orbit (posterior sclera to apex). Goldberg et al7 studied location by quadrant and found that most lesions occur laterally (39%). This was followed closely by superior (32%), medial (20%), and inferior (12%) quadrants.7,8
Specific metastases seem to target certain orbital tissues. Prostate, gastrointestinal, thyroid, and renal tumors often metastasize to bone;, lung to fat; and breast and cutaneous melanoma to fat and muscle. In general, Goldberg7 found tumors tend to metastasize to bone and fat more often than muscle in a 2:2:1 ratio.
Syndromes of Metastatic Orbital Disease
Although the clinical manifestation of an orbital metastasis is related to the primary tumor, it is useful to look at orbital metastases collectively. Based on presenting signs and symptoms, metastatic orbital disease has been divided into five syndromes: solitary mass (66%), infiltrative lesion (24%), inflammatory process (5%), functional deficit (cranial nerve dysfunction out of proportion to other orbital symptoms) (5%), and those that are silent.7,46 Although these lesions rarely present as a purely single syndrome, a dominant presentation is often seen.7,8
Solitary Mass
Most orbital metastases occur as a single mass lesion that causes globe displacement and secondary motility deficits.2,4,5,6,7,8,39 The anterior orbit is often involved,2 and there may be blepharoptosis, loss of vision, and pain.
There are features that suggest specific primary tumors. For example, prostate cancer often metastasizes to the orbital bone and causes an osteoblastic appearance on CT scan. In the terminal stages, a mixed osteoblastic-osteolytic appearance may be seen (3,47) (Fig. 45.1). Renal cell carcinoma also metastasizes to bone; often this is its initial presentation.7,46,48 Solitary renal cell metastasis has occurred up to 20 years after primary diagnosis49 (Fig. 45.2). Thyroid cancer also spreads to bone but it often causes osteolysis.4 Cutaneous melanoma has a preference for orbital fat or extraocular muscle.3,7,50 Endometrial and hepatocellular carcinoma also present as a single mass.51,52,53
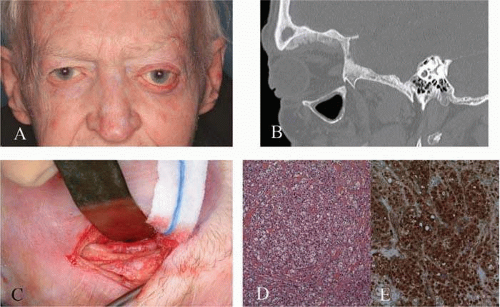 Figure 45.1. Metastatic prostate carcinoma. A. Clinical photograph of an 83- year-old white male who presented with a 3-year history of painless proptosis and mild vertical diplopia. Seven years previously he had been diagnosed with prostate cancer. Visual acuity was limited to 20/100 in each eye because of macular degeneration. Left extraocular movements were limited in all directions; 7mm of left proptosis without inflammatory signs was present. B. Contrast-enhanced CT sagittal reformat image at a bone window and level setting shows osseous proliferation along the orbital roof at the site of subsequently proven metastatic prostate carcinoma. This lesion is osteoblastic as there is proliferation of mineralized bone. C. Incisional biopsy showing abnormal bone and soft tissue. D. Cohesive tumor cells are arranged in a vaguely nested pattern. The nuclei are enlarged (with prominent nucleoli evident on higher power) and there is moderate clear to eosinophilic cytoplasm. (H&E X20.) E. Immunohistochemical stain for prostate-specific antigen (PSA) shows definite cytoplasmic staining confirming the tumor to be of prostatic origin. (PSA IHC X20.) The patient was treated with palliative radiation in addition to hormonal therapy.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|