Otitis media with effusion (OME) describes the persistence of fluid or mucous (glue ear) behind an intact tympanic membrane, usually with no signs of inflammation. If this condition persists for more than three months, it is called chronic otitis media with effusion (COME). Chronic otitis media with effusion is considered to be the most common reason for hearing problems and the most common ear pathology in childhood in general. By the age of 10 years, 80% of all children have gone through at least one episode of COME.1 Treatment options for these diseases vary widely, from watchful waiting to surgery.
Progressive Eustachian tube dysfunction may result in tympanic membrane atelectasis (also, adhesive otitis media), consistent with retractions or invaginations of the tympanic membrane into the middle ear that differ in size, localization, pathogenesis, and biological behavior. Treatment options for atelectasis vary from watchful waiting to small procedures (e.g., tympanostomy tube insertion or adenoidectomy) to intensive surgical procedures, including tympanoplasty and mastoidectomy. Some tympanic membrane retraction pockets resolve spontaneously over time, some remain stable for a long time period, and others develop into an aggressive cholesteatoma with potentially severe complications.
In the following chapter we will suggest a structured treatment guideline for the atelectatic ear with or without effusion according to its clinical presentation and diagnostic workup. However, we should point out that there is no consensus about the best treatment strategy in the literature.2,3,4,5
15.2 Clinical Presentation
Patients with COME and retraction pockets may be asymptomatic for a long time and may not complain about any symptoms in the beginning of the disease process. Adults usually present with a conductive hearing loss when sound-induced movement of the tympanic membrane is restricted due to effusion, adhesion of the tympanic membrane to the ossicles or promontory (▶ Fig. 15.1; ▶ Fig. 15.2; ▶ Fig. 15.3; ▶ Fig. 15.4; ▶ Fig. 15.5), or negative pressure. They will often complain about fullness in the ear. Children may be referred because of delayed speech development (due to a conductive hearing loss), snoring, or recurrent episodes of acute otitis media. An assessment should also be made of possible underlying speech delay or other developmental abnormalities as this may strongly impact decision-making. It should nonetheless be noted that during a routine check-up, deep retraction pockets may be discovered without any problems or complaints having been noted by the patient.
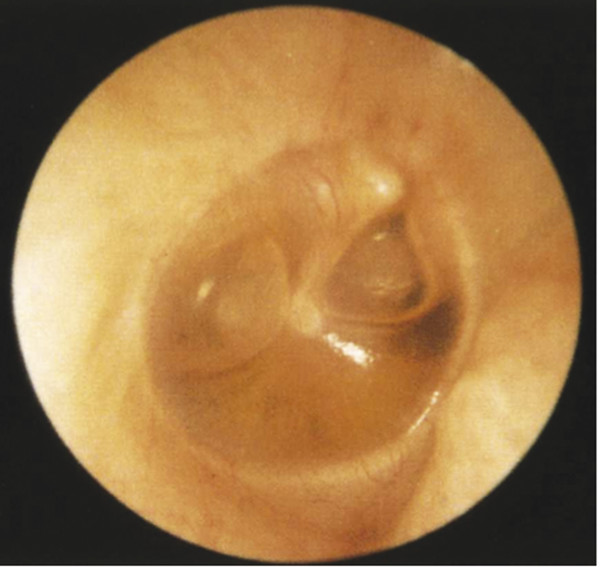
Fig. 15.1 Otitis media with effusion including air-fluid level in right ear.
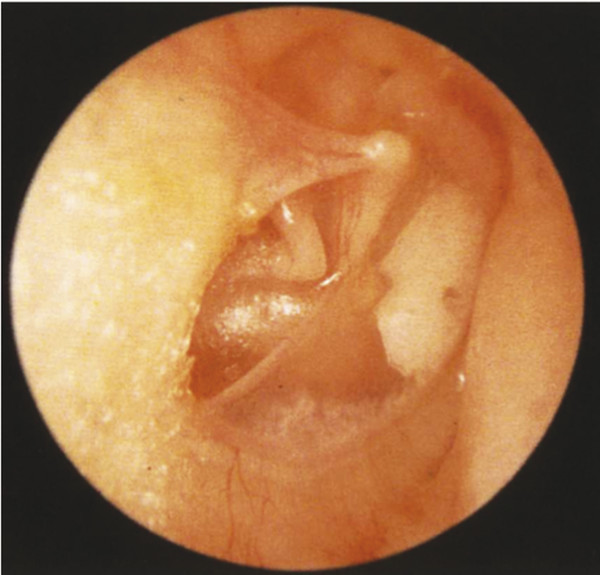
Fig. 15.2 Tympanosclerosis of the anterior pars tensa and fixed retraction of the posterior pars tensa onto the incudostapedial joint and promontory in a right ear.

Fig. 15.3 Epitympanic retraction pocket (left ear). pt, pars tensa tympanic membrane
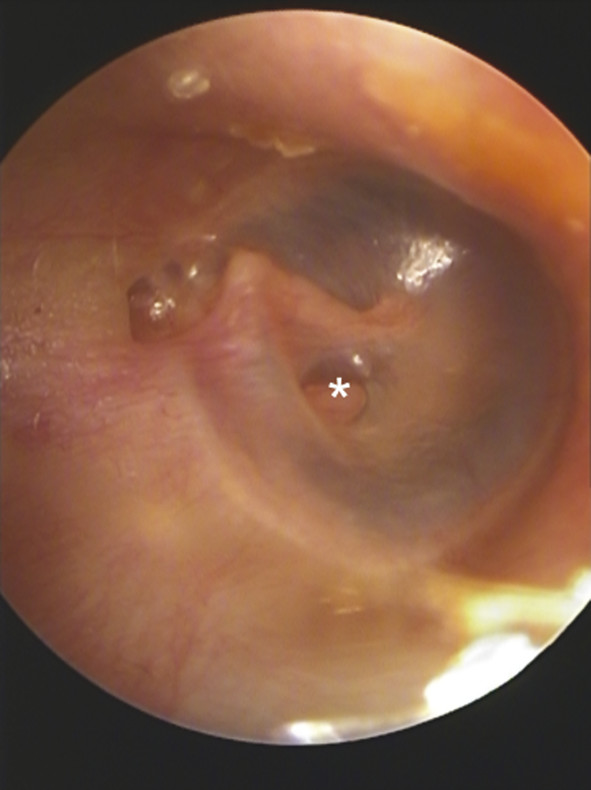
Fig. 15.4 Epitympanic retraction pocket and atelectasis of the pars tensa to the stapes (*) of a right ear.
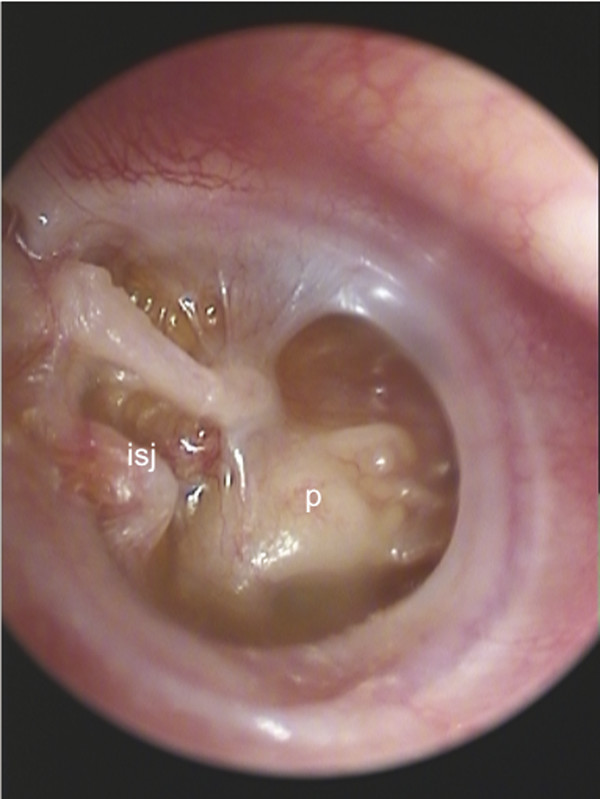
Fig. 15.5 Complete atelectasis of the tympanic membrane (right ear). p, promontory, isj, incudostapedial joint
There are several classifications for retraction pockets, all of which aim to support the physician in giving the correct treatment advice depending on the retraction pocket subtype.6,7,8,9,10,11 These classifications are based on the location of the invagination (pars tensa/pars flaccida), its history (age of the patient in combination with recurrent otitis media with or without otorrhea), its biological behavior (self-cleansing or retaining of epithelial debris; aggressively growing or not changing over several consultations), and the aeration of the middle ear cavity or pneumatization of the mastoid. The most widely accepted classifications are depicted in ▶ Table 15.1; ▶ Table 15.2; ▶ Table 15.3; and ▶ Table 15.4.
Stage | Description |
1 | Tympanic membrane atrophic but not adherent to middle ear structures |
2 | Tympanic membrane adherent to the promontory only |
3 | Tympanic membrane adherent to incus and/or stapes |
4 | Tympanic membrane adherent to ossicles, with deep retraction pocket but without cholesteatoma |
5 | Retraction pocket with cholesteatoma and/or breakthrough |
Used with permission from Borgstein J, Gerritsma TV, Wieringa MH, Bruce IA. The Erasmus atelectasis classification: proposal of a new classification for atelectasis of the middle ear in children. Laryngoscope. 2007; 117(7):12551259 | |
Grade | Description |
1 | Retracted tympanic membrane which does not touch any middle ear structures |
2 | Retracted tympanic membrane touches the stapes or incus |
3 | Retracted tympanic membrane down to promontory |
4 | Retracted tympanic membrane into sinus tympani with collected keratin |
Used with permission from Sadé J, Berco E. Atelectasis and secretory otitis media. Ann Otol Rhinol Laryngol. 1976; 85 Suppl 25:66–72. | |
Grade | Description | Typical Treatment |
1 | Drum collapse without hearing loss | Observation or tympanostomy tube |
2 | Drum collapse with hearing loss but no ossicular dysfunction | Tympanoplasty |
3 | Drum collapse with hearing loss and ossicular dysfunction | Tympanoplasty with ossicular chain reconstruction |
4 | Deep retraction with hearing loss and cholesteatoma | Tympanomastoidectomy or epitympanectomy |
Note: If an effusion is present, add an asterisk (*) to indicate a possible long term poor hearing prognosis: e.g., Stage II* for an severe collapse with an effusion. Data from Black B. Reporting Results in Ossiculoplasty. Otol Neurotol. 2003; 24 (4) 534-542. | ||
Grade | Description |
1 | Slight dimpling of the pars flaccida |
2 | Retraction to malleus neck; entire pocket is visible |
3 | Partly hidden retraction with possible erosion of the scutum |
4 | Deep retraction with definite scutal erosion; pocket is not entirely visualized |
Used with permission from Tos M, Poulsen G. Attic retractions following secretory otitis. Acta Otolaryngol. 1980;89:479–486. | |
The proposed pathogenesis of atelectasis or adhesive otitis media is similar to that for the origin of COME.1,12 It is based on the “ex vacuo” theory published by Politzer in 1867,13 where a negative pressure in the middle ear cavity is induced by a dysfunction of the Eustachian tube and is followed by inflammation and edema of the mucosal membranes of the Eustachian tube and middle ear cavity in combination with an epithelial proliferation as a reaction to the chronic inflammation.14 The particular impact of the responsible preconditions is still under discussion, but the combination of retraction and proliferation for the development of cholesteatomas are the most accepted theories of pathogenesis to date.14
15.3 Diagnostic Tests
In addition to taking a specific medical history, the most important diagnostic tool is the microscopic examination of the tympanic membrane. In young children, cerumen or debris may sometimes not allow a reliable evaluation of the tympanic membrane; therefore, cleaning of the ears under general anesthesia may be required. In older children and adults, the entire tympanic membrane can usually be examined and evaluated with regard to retraction pocket size and location, whether the eardrum is fixed to the promontory/ossicles while performing the Valsalva maneuver, or if there is effusion.
Whereas otoacoustic emissions and tympanometry can be performed even in newborns, pure tone audiometry is usually not possible until the age of four years. Mild to severe conductive hearing loss can be observed in patients with atelectasis of the tympanic membrane, depending on retraction pocket size, effusion viscosity, or erosion of the ossicles. There is no reliable direct correlation of the conductive hearing loss and the severity of the disease. Especially in patients with mild hearing loss, the air conduction threshold may be less before removing the retraction pocket and scar tissue due to a sheeting effect, even for an eroded ossicular chain.
Tympanometry is routinely performed in a clinical workup of most otology patients. Whereas tympanometry is considered an easy method for measuring middle ear pressure, significant differences between the values read from the tympanogram and those measured by direct puncture of the tympanic membrane do exist. Tympanometry in ears with retracted or partially atelectatic tympanic membranes do not reflect the true middle ear pressure. The position of the tympanogram peak depends on the size of a retraction pocket and the remaining middle ear gas volume.15 Nevertheless, if the tympanic membrane is not severely retracted, tympanometry is quite useful in the diagnosis of COME, with a sensitivity of about 93% and a specificity up to 70%.16,17
Dysfunction of the Eustachian tube can be caused by adenoid hypertrophy or nasal obstruction due to various underlying pathologic conditions (e.g., hyperplasia of the turbinates, retention cysts of the nasopharynx, nasopharyngeal tumors, etc.). Therefore, an endoscopic examination of the nose should be included at least once in routine workup when chronic ear problems are present.
Imaging is not necessarily required for routine cases of atelectasis or COME. High-resolution computed tomography (CT) scan of the temporal bone is recommended in advanced cases where a cholesteatoma may be suspected or if there is any sign of an underlying chronic ear diseasecomplication.
There are high-risk groups of children with reduced Eustachian tube function for example, cleft palate patients, patients with Down syndrome or primary ciliary dyskinesia, as well as immunocompromised patients. These patients need a broader interdisciplinary workup involving pediatricians, oral surgeons, geneticists, and pediatric audiologists.
15.4 Treatment Decision-Making
In the following section, different clinical criteria are discussed with regard to their impact on whether or not to pursue a more conservative treatment or a surgical option. None of these criteria are a determining factor on their own, but each should be evaluated in the context of other findings (presented as a summary in ▶ Table 15.5).18
Watchful waiting | Surgical treatment |
Entire retraction pocket can be visualized completely by microscopic examination | Entire retraction pocket cannot be visualized completely by microscopic examination |
Conductive hearing loss <20 dB SPL | Conductive hearing loss >20 dB SPL |
No otorrhea | Recurrent otorrhea |
Good pneumatization | Poor pneumatization |
Normal Eustachian tube function | Disturbed Eustachian tube function |
Adult patient | Pediatric patient |
Pars flaccida | Pars tensa |
No progression | Progression |
Poor medical conditions | Social criteria |
SPL, sound pressure level | |
15.4.1 Microscopic Examination Findings
Microscopic examination of the tympanic membrane allows one of the most important decision-making criteria. In cases where the retraction pocket cannot be completely visualized through the microscope, the use of an angled endoscope can be helpful.19,20 A self-cleansing retraction pocket without any noticeable or measurable symptoms usually does not need immediate surgical treatment. When a retraction pocket is filled with debris and/or cannot be completely visualized, a surgical treatment may be recommended. When examining tympanic membrane atelectasis, the presence of aeration within the protympanum may predict a good hearing result with tympanoplasty in that the tympanic membrane may be bound by adhesions to the underlying middle ear cleft in spite of subsequent recovery of Eustachian tube function (▶ Fig. 15.6).
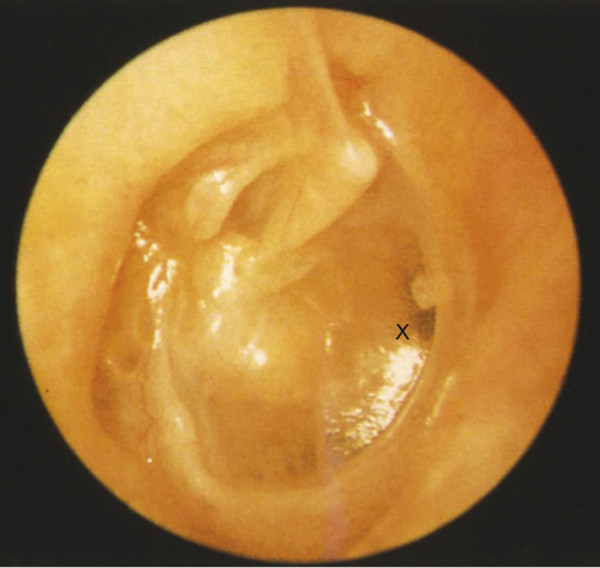
Fig. 15.6 Retraction of the posterior pars tensa of a right ear onto the incudostapedial articulation, which has been eroded and replaced by a fibrous band. Despite the retraction, note the presence of air in the anterior mesotympanum and protympanum (X), which suggests some degree of recovered Eustachian tube function.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


