Purpose
To evaluate visual and refractive outcomes after implantation of a trifocal intraocular lens (IOL).
Design
Prospective, nonrandomized noncomparative case series.
Methods
setting : Department of Ophthalmology, Goethe University, Frankfurt/Germany. patient or study population : Twenty-seven patients (54 eyes) who had bilateral implantation of the AT LISA trifocal IOL (AT LISA tri839MP; Carl Zeiss Meditec, Jena, Germany) pre-enrollment. Exclusion criteria were previous ocular surgeries excluding cataract surgery and refractive lens exchange, irregular corneal astigmatism of >1.5 diopter, and ocular pathologies or corneal abnormalities. Intervention or Observation Procedure(s) : Postoperative examination at 1 and 3 months included manifest refraction; monocular and binocular uncorrected (UCVA) and distance-corrected (DCVA) visual acuity in 4 m, 80 cm, and 40 cm; slit-lamp examination; and tomography. At 3 months defocus testing, binocular contrast sensitivity (CS) under photopic and mesopic conditions, and a questionnaire on subjective quality of vision, optical phenomena, and spectacle independence were performed. Main Outcome Measure(s) : Three-months-postoperative monocular and binocular UCVA and DCVA in 4 m, 80 cm, and 40 cm (logMAR); defocus curve; CS; and quality-of-vision questionnaire results.
Results
Mean spherical equivalent was 0.05 ± 0.32 D 3 months postoperatively. Binocular UCVA at distance, intermediate, and near was −0.1 ± 0.1 logMAR, 0.0 ± 0.1 logMAR, and 0.0 ± 0.1 logMAR, respectively. Despite some optical phenomena, 92% of patients would choose the same IOL again.
Conclusion
Evaluation of a trifocal IOL showed good VA (0.1 logMAR or better) at far, intermediate, and near distance; high patient satisfaction despite some optical phenomena; and high spectacle independence 3 months postoperatively.
Existing bifocal lenses have been proven to offer a broad range of vision with increased spectacle independence when compared with a monofocal intraocular lens (IOL). Patients after implantation of multifocal lens showed more spectacle independence compared to monofocal lens with low monovision but were more likely to suffer from dysphotopsia. However, a contradictory study showing that monovision with monofocal lens can provide comparable good distance and near vision and more favorable intermediate and computer vision with less symptomatic glare and halos than multifocal IOLs has also been published.
Bifocal IOLs with reduced near addition of +3.0 diopter (D) showed improved intermediate visual acuity (VA) when compared to +4.0 D add power while providing comparable distance (DVA) and near visual acuity (NVA). However, these bifocal IOLs still show limitations at intermediate distance. Intermediate vision is becoming increasingly important for those patients undergoing cataract surgery or refractive lens exchange as a consequence of the role computers play in our lives today. Recently, bifocal IOLs with decreased near add of below +3.0 D have been developed to further improve intermediate VA, thus showing limitations at near distance.
As one of the first trifocal IOLs, the AT LISA tri 839MP (Carl Zeiss Meditec, Jena, Germany) aims to provide a broader range of spectacle independence than bifocal IOLs as the light is distributed into 3 foci: distance, intermediate, and near. The additions are +3.33 D for near (40 cm) and +1.66 D for intermediate (80 cm), respectively. The corresponding additions projected on the spectacle plane are +2.50 D and +1.25 D, respectively.
The purpose of this study was to evaluate various visual demands and refractive outcomes, subjective quality of vision in daily life activities, and spectacle independence following trifocal IOL implantation (AT LISA tri 839MP).
Methods
This prospective single-arm study was conducted from April 9 th 2013 to July 14 th 2014 in compliance with Good Clinical Practices (GCP), including International Harmonization (ICH) Guidelines and consistent with the tenets outlined in the Declaration of Helsinki. The Goethe University, Frankfurt Ethics Committee approval was obtained prior to patient enrollment.
Fifty-four eyes of 27 subjects were enrolled after bilateral phacoemulsification and implantation of a trifocal IOL (AT LISA tri839MP; Carl Zeiss Meditec, Jena, Germany) into the capsular bag. In all cases, the Haigis formula was used for the calculation of the IOL power to implant according to the measurements of corneal power, axial length, and anterior chamber depth obtained with the IOL-Master (IOL-Master 5000; Carl Zeiss Meditec). IOL power (mean ± standard deviation [SD] [range]) was 18.74 ± 5.64 D (6; 27.5 D). Mean target refraction was −0.2 ± 0.1 D. The surgery was not part of the study, as we enrolled patients postoperatively. All surgeries were performed under topical anesthesia by 1 experienced surgeon (T.K.). Capsulotomies, lens fragmentation, and corneal incisions were done using the LenSx femtosecond laser (Alcon Laboratories, Inc, Fort Worth, Texas, USA) in 46 eyes of 23 patients. Manual capsulorrhexis and ultrasound lens fragmentation were performed in 8 eyes of 4 patients. Phacoemulsification was performed using standard ultrasound technique (Infiniti; Alcon Laboratories, Inc). In all cases, the corneal incision was located on the preoperative steep meridian of the corneal astigmatism.
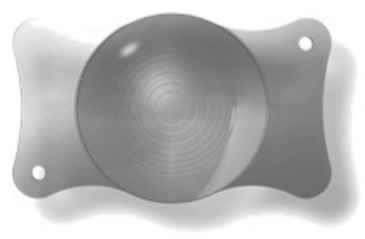
The AT Lisa tri is a preloaded IOL with a single-piece diffractive multifocal design. It has a 6.0 mm biconvex optic with an overall length of 11.0 mm, a central trifocal zone over a diameter of 4.34 mm, and a peripheral bifocal zone from 4.34 mm to 6 mm. It is made of hydrophilic acrylic (25%) with a hydrophobic surface and a unique asymmetrical light distribution of 50%, 20%, and 30% between far, intermediate, and near foci. The available dioptric power ranges from 0.0 D to +32.0 D in 0.5 D increments ( Figure 1 ).
All patients recruited had undergone bilateral cataract surgery or refractive lens exchange, receiving a trifocal IOL with the described procedures prior to study enrollment; had a regular corneal astigmatism of <1.5 D postoperatively measured with the Pentacam (Oculus, Wetzlar, Germany); and signed an informed consent form. Toric trifocal IOLs were not implanted. Exclusion criteria were previous ocular surgeries except for cataract surgery or refractive lens exchange, ocular pathologies, corneal abnormalities, and endothelial cell count below 2000/mm 2 .
Primary efficacy endpoints were assessed 3 months after the second eye surgery and included binocular uncorrected and distance-corrected VA at far (4 m), intermediate (80 cm), and near (40 cm) distance, as well as patient satisfaction. Examination at 1 and 3 months postoperative visits included manifest refraction using the 100% contrast Early Treatment Diabetic Retinopathy Study (ETDRS) chart under photopic lighting conditions (167 cd/m 2 ); monocular and binocular uncorrected and distance-corrected VA at 4 m, 80 cm, and 40 cm under photopic lighting conditions, given in logMAR (ETDRS); and an examination of anterior and posterior eye segment (slit lamp) and tomography (Pentacam).
At the 3-month visit additional measurements were performed. Defocus testing was conducted monocularly, distance-corrected with defocus from −4.0 D to +1.5 D in 0.5 D increments (ETDRS) under photopic lighting conditions. Binocular contrast sensitivity (CS) was measured under photopic, mesopic (0.167 cd/m 2 ), and mesopic with glare lighting conditions using the “Frankfurt-Freiburg Contrast and Acuity Test System” (FF-CATS). Results were compared to a monofocal aspheric IOL study. Patients completed a short quality-of-vision questionnaire. The questionnaire is a subjective, intuitive test, which was developed to evaluate quality of vision after refractive surgery. By answering the questionnaire, the patient provides his or her subjective assessment concerning optical phenomena. Patients were asked about their perception of optical phenomena (halo, starburst, double vision) and spectacle independence at far, intermediate, and near distance. On a scale from 1 (very good) to 6 (very bad), patients rated overall their subjective quality of vision for different daily life tasks. Furthermore, they were asked if they would choose the same IOL again and if they would recommend the IOL to others.
Results
The mean patient age was 64 ± 7.9 years (51; 77 years) and 63% (17 of 27) were female. Cataract surgery was performed in 30 eyes and refractive lens exchange in 24 eyes. Spherical equivalent (SE) changed from -1.60 ± 4.19 D (−9.63; 4.75 D) preoperatively to 0.05 ± 0.32 D (−1.00; 0.75 D) 3 months postoperatively. At the 3 months postoperative visit 80% of all eyes showed SE accuracy of ±0.5 D ( Figure 2 ). Astigmatism decreased from 0.72 ± 0.70 D (0.00; 4.50 D) to 0.32 ± 0.33 D (0.00; 1.25 D).
At the 3 month visit monocular uncorrected corrected VA was 0.01 ± 0.10 logMAR at 4 m, 0.06 ± 0.12 logMAR at 80 cm, and 0.09 ± 0.12 logMAR at 40 cm. Monocular distance-corrected VA was −0.04 ± 0.08 logMAR at 4 m, 0.04 ± 0.11 logMAR at 80 cm, and 0.06 ± 0.13 logMAR at 40 cm. Binocular uncorrected VA was −0.06 ± 0.10 logMAR at distance, 0.00 ± 0.12 logMAR at intermediate, and 0.04 ± 0.10 logMAR at near distance. Binocular distance-corrected VA was −0.1 ± 0.09 logMAR at 4 m, −0.01 ± 0.10 logMAR at 80 cm, and 0.02 ± 0.11 logMAR at 40 cm ( Table 1 ).
| Parameters | 1 Month | 3 Months | ||||||
|---|---|---|---|---|---|---|---|---|
| Monocular | N (Eyes) | Binocular | N (Subjects) | Monocular | N (Eyes) | Binocular | N (Subjects) | |
| UDVA (mean ± SD) | 0.01 ± 0.11 | 50 | −0.06 ± 0.09 | 25 | 0.01 ± 0.10 | 54 | −0.06 ± 0.10 | 27 |
| CDVA (mean ± SD) | −0.02 ± 0.20 | 50 | −0.09 ± 0.10 | 26 | −0.04 ± 0.08 | 51 | −0.10 ± 0.09 | 27 |
| UIVA (mean ± SD) | 0.03 ± 0.11 | 52 | −0.01 ± 0.10 | 25 | 0.06 ± 0.12 | 54 | 0.00 ± 0.12 | 27 |
| DCIVA (mean ± SD) | 0.06 ± 0.21 | 48 | −0.03 ± 0.10 | 25 | 0.04 ± 0.11 | 51 | −0.01 ± 0.10 | 27 |
| UNVA (mean ± SD) | 0.10 ± 0.13 | 52 | 0.03 ± 0.11 | 26 | 0.09 ± 0.12 | 54 | 0.04 ± 0.10 | 27 |
| DCNVA (mean ± SD) | 0.07 ± 0.13 | 48 | 0.03 ± 0.12 | 25 | 0.06 ± 0.13 | 51 | 0.02 ± 0.11 | 27 |
Cumulative binocular distance-corrected VA results are shown in Figures 3–5 . All patients had a CDVA of 0.10 logMAR or better 3 months postoperatively. Twenty-six patients (96%) had a CDVA of 0.00 logMAR or better ( Figure 3 ). Distance-corrected intermediate VA was 0.20 logMAR or better in 27 subjects (100%), 0.10 in 25 subjects (93%), 0.00 logMAR or better in 19 (70%), and −0.10 logMAR or better in 13 patients (48%) ( Figure 4 ). Twenty-four patients (89%) had a distance-corrected NVA of at least 0.10 logMAR and 17 (63%) at least 0.00 logMAR or better.
Monocular defocus curve at 3 months showed best VA (−0.05 logMAR and 0.06 logMAR) with defocus of 0.00 D and −2.50 D, simulating distances of 4 m and 40 cm. In between these 2 peaks VA became worse (0.18 logMAR) with add power of −2.0 D (50 cm) ( Figure 6 ). CS measured photopic, mesopic, and mesopic with glare was 1.58 ± 0.57, 0.96 ± 0.31, and 0.98 ± 0.48 logCS, respectively. We compared these results to a monofocal aspheric IOL ( Figure 7 ).



