Purpose
To determine the ability of optical coherence tomography (OCT) angiography to image the microvascular structures compared with fluorescein angiography (FA) in patients with macular edema associated with branch retinal vein occlusion (BRVO).
Design
Retrospective, observational, consecutive case series.
Methods
Twenty-eight eyes of 27 patients (14 men, 13 women; mean age, 68.4 years) with macular edema associated with BRVO were enrolled. Simultaneous OCT angiography and FA were performed in all patients to evaluate the microvascular abnormalities and nonperfused areas.
Results
OCT angiography detected nonperfused areas in 28 eyes and FA in 18 eyes. The respective findings of superficial capillary telangiectasias by OCT angiography and FA were 13 and 11 eyes, for deep capillary telangiectasias 28 eyes and 11 eyes, for collateral vessels 18 eyes and 16 eyes, and for microaneurysms 13 eyes and 14 eyes. OCT angiography facilitated differential layer analysis of microaneurysms and collaterals as well as capillary telangiectasias in the retina.
Conclusions
OCT angiography can visualize microvascular abnormalities equally well or better than FA in eyes with BRVO. Multimodal imaging using OCT angiography and FA can be a powerful tool to evaluate the pathology in BRVO.
Branch retinal vein occlusion (BRVO) usually results from a thrombus at the arteriovenous crossings where a thickened artery compresses the underlying venous wall, resulting in elevated venous pressure and consequent macular edema, retinal ischemia, and rupture of the retinal wall with intraretinal hemorrhage. In the chronic phase, after absorption of the intraretinal hemorrhage, there are several retinal vascular abnormalities, such as capillary nonperfusion, capillary dilation, microaneurysms, telangiectatic vessels, and collateral vessels.
Fluorescein angiography (FA) is useful to confirm the diagnosis of BRVO and evaluate complications. The characteristic findings on FA are delayed filling of the occluded retinal vein, capillary nonperfusion, microaneurysms, and dye extravasation from macular edema or retinal neovascularization. Ultra-wide-field FA using the Optos 200Tx (Optos PLC, Dunfermline, Scotland, UK) shows nonperfused areas in the peripheral retina. However, dense retinal hemorrhages and/or macular edema make interpretation of FA images difficult because of blocked or pooled fluorescein. In addition, FA does not visualize the deeper capillary network in the retina well, possibly because of light scattering in the retina.
Optical coherence tomography (OCT) is a rapid, noninvasive technique that provides high-resolution retinal images. Recently, 3-dimensional and noninvasive vascular mapping without dye was accomplished using OCT angiography. OCT angiography has the advantage of 3-dimensional noninvasive vascular mapping in the retina and choroid in just a few seconds, thus displaying several vascular layers (ie, the superficial and deep capillaries, outer retina, and choriocapillaris). Recently, de Carlo reported the microvascular changes in patients with BRVO. We evaluated the ability of OCT angiography to visualize several vascular abnormalities and compared the findings with conventional FA.
Methods
Study Design and Setting
This was a retrospective, observational, consecutive case series conducted in an institutional setting. The study design was approved by the Institutional Review Board of Nagoya City University Graduate School of Medical Sciences. All patients provided written informed consent for participation in the study. The described research methods and analysis adhered to the tenets of the Declaration of Helsinki.
This study was conducted at Nagoya City University Hospital from November 1, 2014 through May 31, 2015. Twenty-eight eyes of 27 patients (14 men, 13 women; mean age, 68.4 years; range, 41–86 years) with macular edema associated with BRVO were enrolled. The mean follow-up period was 28.8 months (range, 4–122 months). All patients underwent a complete ophthalmic examination including measurement of best-corrected visual acuity, indirect ophthalmoscopy, fundus photography, OCT (Cirrus HD-OCT; Carl Zeiss Meditec, Jena, Germany), OCT angiography (RTVue XR Avanti, AngioVue; Optovue Inc, Fremont, California, USA), and/or FA. FA was performed using the wide-field laser ophthalmoscope Optos 200Tx and/or confocal scanning laser ophthalmoscopy (Heidelberg Retina Angiograph 2 [HRA2]; Heidelberg Engineering, Heidelberg, Germany). OCT angiography and FA also were performed on the same day. The mean measurement time of OCT angiography and FA was 25.1 months (range, 1–120 months) after disease onset. The incidence rates of nonperfused areas, superficial and deep capillary telangiectasias, collateral vessels, and microaneurysms were determined using OCT angiography and FA. Patients whose OCT angiography images were of inadequate quality for evaluation because of eye movement or cataract or who had not undergone FA because of renal and/or liver dysfunction or allergy to fluorescein were excluded.
Optical Coherence Tomography Angiography
OCT angiography images were obtained using the RTVue XR Avanti AngioVue with a split-spectrum amplitude-decorrelation angiography algorithm, as previously described. The instrument obtains 70 000 A-scans/second, using a light source centered on 840 nm; the tissue resolution is 5 μm in depth and 15 μm in width. Two consecutive B-scans (M-B frames) were captured at a fixed position before proceeding to the next sampling position, split into 11 decorrelation sets, compared to detect motion, and merged. The merging of the sets increased the signal-to-noise ratio and provided the high-detail, motion contrast “angioflow” image.
Results
Nonperfused Areas
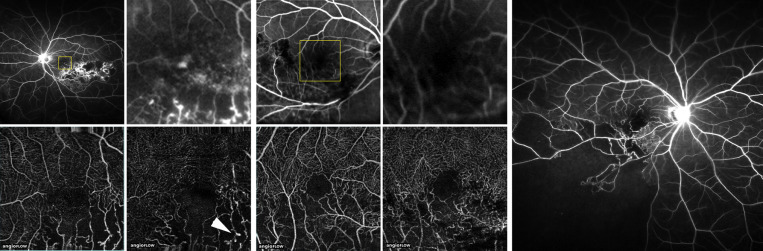
OCT angiography detected nonperfused areas in all 28 eyes compared with FA, which detected them in 18 eyes. In some FA images, the nonperfused areas were masked by hyperfluorescence from the leaking vessels or hypofluorescence due to retinal hemorrhage ( Figure 1 ), whereas OCT angiography detected them clearly because of the absence of fluorescein dye. OCT angiography also visualized the nonperfused areas clearer than FA ( Figure 1 ) and was superior for differentiating the foveal avascular zone from nonperfused areas because the OCT angiography system provided higher-resolution images than FA. OCT angiography did not detect nonperfused areas in the peripheral retina. However, the Optos 200Tx visualized the nonperfused areas in the peripheral retina ( Figure 1 ).
Superficial Capillary Telangiectasia
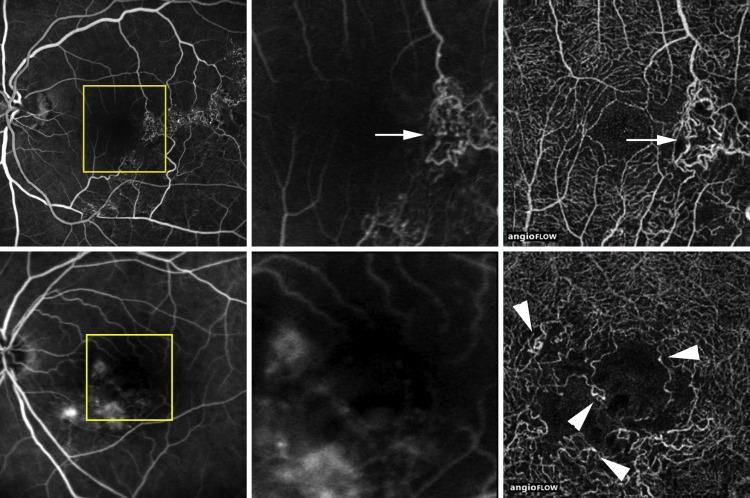
OCT angiography detected superficial capillary telangiectasia in 13 of 28 eyes, vs FA in 11 eyes; even with high-resolution confocal scanning laser ophthalmoscopy HRA2 imaged the superficial capillary telangiectasia in 11 eyes maximally, but it was difficult to observe the normal capillary network in the superficial capillary layer ( Figure 2 ). OCT angiography detected even the very thin capillary networks in the superficial layer ( Figure 2 ).
Deep Capillary Telangiectasia
OCT angiography detected deep capillary telangiectasia in all 28 eyes, vs FA in 11 eyes. On FA, the deep capillary network was barely visible because of the 2-dimensional image photography and blockage by choroidal vessels ( Figure 2 ). OCT angiography easily detected the capillary telangiectasia and the normal capillary networks in the deep layer ( Figure 2 ).
Collateral Vessels (Venovenous Shunt)
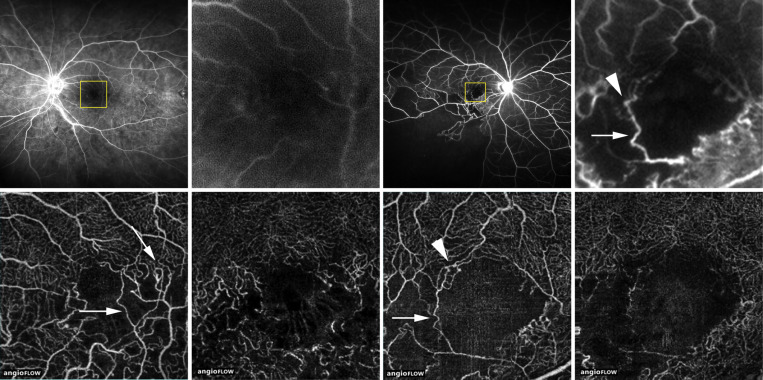
OCT angiography detected collateral vessels in 18 eyes, vs FA in 16 eyes. Pre-existing collateral vessels that connected adjacent venous beds were distended and carried more blood, which tended to decrease the retinal venous pressure in the occluded segment. The collateral vessels were present where the occlusive vein was connected to another vein ( Figure 3 ) or a normal (circulated) vein that traversed the nonperfused retina ( Figure 3 ). OCT angiography facilitated differential layer analysis of the collateral vessels ( Figure 3 ) and showed that the collateral vessels were in the superficial and deep layers in all 18 eyes. FA did not clarify the location of the collateral vessels with differential layer analysis in the retina ( Figure 3 ).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


