(1)
Narayana Hridayalaya Multispeciality, Bangalore, India
Approximately 50–60 % cases of head and neck cancer present in advanced stage in developing world. The conventional TNM staging considers only limited factors, and it is not feasible to group every advanced cancer in the same group. There are various factors that predict biological behavior that can be of great help in treating these tumors. The treatment of such cases needs clear philosophy, and choices need to be rational to avoid catastrophic outcome. These patients are often miserable due to constant pain, fungation, and bleeding and deserve good care. Majority of these patients are treated with palliative intent considering them either inoperable or borderline operable without actually considering possibility of cure. It is also essential to realize that these patients are actually at very advanced stage and surgery remains the only realistic chance of cure. Any other treatment including chemoradiotherapy essentially remains a palliative option. We have developed a rational approach to treat these patients that is discussed in this chapter.
Guidelines for Very Advanced Cases
The conventional classification system stages all cases of T4 in one group, and this doesn’t help in treatment decision planning. It is important to assess these patients individually and also to have some rational guidelines to maintain consistency in treatment. We follow the guideline demonstrated in Fig. 14.1. The aim is to assess biology of disease and prognosis of patient before deciding on treatment options. The cases that present de novo have best prognosis, while patients with recurrent disease have inferior outcome. Many patients present with inappropriate first treatment and they actually fare better compared to recurrent disease that came back after complete treatment. The primary tumors can be broadly classified in two sections. The one class of patients has large primary disease with very limited nodal disease (gingivo-buccal sulcus, PNS), and this indicates aggressive disease at local site with limited tendency to distant spread. We prefer to offer aggressive surgical option to this group and have obtained very good long-term results. The other group with large nodal disease has high tendency for regional and distant failure, and this fact should be kept in mind while making treatment selection. The palliative surgery has an important role for select group of patients who has limited local disease that is affecting their quality of life (QOL) and can be addressed by simple surgical procedure. It is important to remember what you wish to palliate while making such choice.
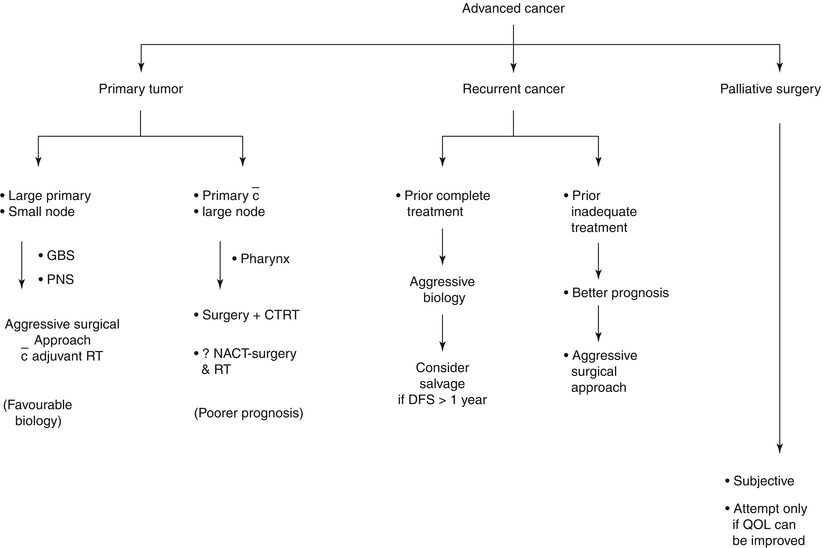
Fig. 14.1
Advanced head and neck cancer – concepts for treatment approach
Tumors Without Previous Treatment
These patients have the best prognosis among all advanced cancers. They can be grouped broadly into two, one of which has favorable biology than the other. Few subsites like gingivo-buccal sulcus cancer and PNS cancer have a tendency to grow locally with limited nodal spread, and these patients have good outcome if local treatment is adequate. The other group where large nodal mass is the main presentation has high rate of regional and distant failure and one needs to have rational approach for their treatment. Even with their comparably poor outcome, surgery remains the mainstay treatment for truly advanced cancers.
Achieving negative three-dimensional margins remains the most important prognostic factor for patients receiving surgery. This holds true even for very advanced cancers. The concept of compartment surgery applies for these tumors as discussed in this book. This concept has added consistency in achieving negative margins for large tumors involving soft tissue at depth. All the surgeons treat cases like these in their practice and have reasonable results. They would treat them more aggressively and consistently if an approach delivers negative margins regularly. The aim of any surgery is to achieve good local control and if one can remove all cells with potential to harbour cancer cells, this can be achieved. The concept of compartment resection has been practiced for about 5 years in our institute, and we feel confident about achieving good local control in majority of these cases. Improved options for reconstruction with microvascular technique have made these approaches more feasible.
The treatment of advanced and complex cases needs different considerations for each site. These are discussed in subsequent sections:
Buccal mucosa and alveolus cancer
Tongue and floor of mouth cancer
Oropharynx cancer
Neck cancer
Buccal–alveolus complex cancer
Cancer with extensive skin infiltration and surrounding edema
High ITF with extensive skin involvement
Patient requiring double flap reconstruction

Fig. 14.2
Patient with extensive skin infiltration, involving the entire upper and lower lip with surrounding edema. This is an inoperable case for majority of centers. It is interesting to note that it doesn’t involve any structures that are strictly nonremovable and he has no neck nodes. If we can remove the entire tumor with negative margins, we may have good outcome

Fig. 14.3
Resected specimen with adequate skin margins. Always try to include surrounding edema and redness in resection margin
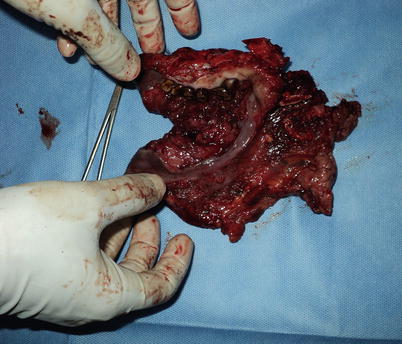
Fig. 14.4
Adequate mucosal margins are shown in the specimen

Fig. 14.5
Photograph shows completed resection

Fig. 14.6
Proposed PMMC flap. The donor site would need STG

Fig. 14.7
Outcome after 10 days of procedure. The feeding tube is out and the patient can take semisolid food

Fig. 14.8
Oral continence is acceptable for such disease. This patient is disease free for 1 year (last follow-up). There is a chance that these patients may develop skin nodules, but the incidence is very rare in patients who have not received any treatment before. The incidence of distant metastasis for N0 neck is also not very high

Fig. 14.9
A case with extensive skin fungation, disease going beyond the zygoma and involving high ITF

Fig. 14.10
Proposed resection with adequate margins. Intracranial involvement and involvement of prevertebral fascia and carotid artery are the only contraindications for us not to offer treatment to any patient
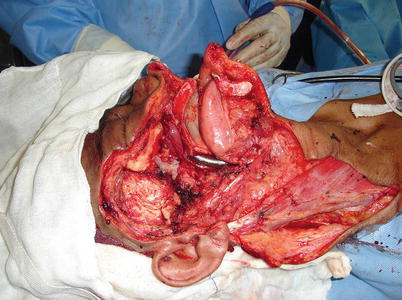
Fig. 14.11
Compartment resection with clear margins

Fig. 14.12
ALT flap reconstruction. She defaulted for adjuvant radiotherapy (RT) and developed opposite node after 6 months and died of distant metastasis. She didn’t have local recurrence till she died and had good QOL

Fig. 14.13
A verrucous type of cancer involving extensive skin and anterior arch of the mandible. He requires two flap reconstruction

Fig. 14.14
The resection includes angle to angle mandible with skin. The focus of reconstruction would be to provide support to anterior tongue and FOM

Fig. 14.15
The resected specimen showing adequate margins
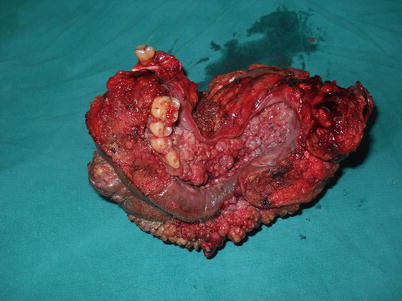
Fig. 14.16
The specimen with adequate mucosal margins

Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


