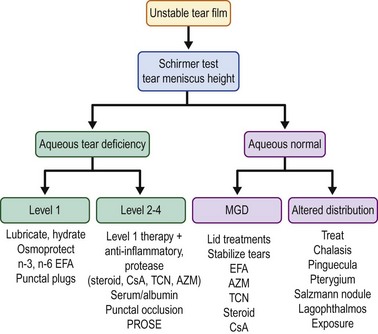
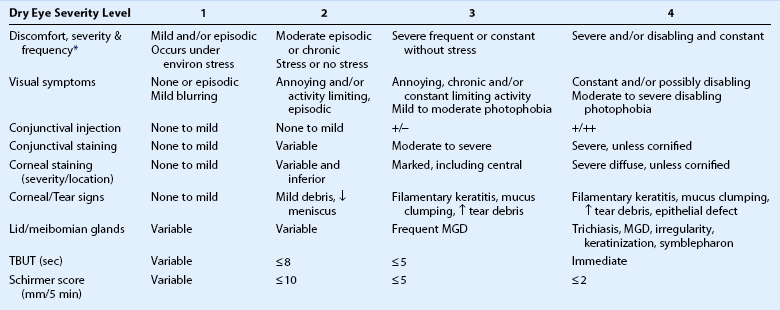
12 Dry eye develops when disease or dysfunction of one or more components of the integrated lacrimal functional unit is no longer able to maintain a stable tear film.1 Dry eye is a common condition with a reported prevalence ranging from 2% to 14.4%.2–6 Patients with dry eye typically complain of eye irritation, such as foreign body sensation, burning, and dryness, as well as visual symptoms, including photophobia and fluctuating vision. Dry eye causes pathological changes to the ocular surface epithelium with disruption of corneal epithelial barrier function and loss of mucus-secreting goblet cells. Dry eye may decrease quality of life, and in the most severe cases, dry eye disease can cause functional and occupational disability. The impact of dry eye on quality of life was rated to be equivalent to unstable angina using utility assessments.7 Therapy of dry eye is aimed at improving irritation symptoms, visual quality and sight-threatening corneal epithelial disease. This chapter reviews current evidence and consensus-based treatment recommendations for dry eye, that are based on previously published recommendations of the International Dry Eye Workshop (DEWS) and Meibomian Gland Workshop.8,9 Optimal management of dry eye or tear dysfunction requires performance of a minimal number of diagnostic tests to: identify character, frequency and severity of patient complaints; confirm presence of an unstable tear film; identify aqueous tear deficiency; detect meibomian gland disease; identify conditions altering tear clearance and/or distribution (conjunctivochalasis, lid or punctal ectropion, punctal stenosis, pterygium, pingueculum, Salzmann’s nodular degeneration) and detect location and extent of ocular surface epithelial disease. Results of these tests, combined with clinical impressions, can be used to grade disease severity. The Dry Eye Workshop proposed four levels of severity (Table 12.1);8 however, disease severity may be better characterized on a continuous spectrum. Table 12.1 Severity Grading Scheme for Dry Eye eviron: environmental; MGD: meibomian gland disease. *Discomfort symptoms may be minimal or absent in levels 3 and 4 due to nerve degeneration. Modified from scheme proposed by Dry Eye Workshop (Pflugfelder S (committee chairman) Management and therapy of dry eye disease: report of the Management and Therapy Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf 2007;5:163–78.) Aqueous deficiency requires therapies to minimize or eliminate environmental factors, lubricate and hydrate the ocular surface, protect against osmotic stress and stimulate tear production. Replacement of tear constituents with autologous serum or plasma and protection of the ocular surface with therapeutic contact lens, such as PROSE are necessary in more severe cases (levels 3 and 4). Ocular surface inflammation is a pathological feature shared by aqueous deficient and aqueous sufficient dry eye conditions and many currently utilized therapies, inhibit production of inflammatory cytokines and proteases. A severity-based treatment algorithm for treatment of dry eye is presented in Figure 12.1. Therapies can be added or removed based on objective and subjective response. Systemic and environmental factors contributing to dry eye should be modified or eliminated. Systemic medications with anticholinergic side effects (e.g. antihistamines, antidepressants, and antispasmodics) should be eliminated if possible. Exposure to desiccating environmental stresses (e.g. low humidity and air conditioning drafts) that cause irritation symptoms or increase tear evaporation, should be minimized or eliminated. The height of video display terminals should be adjusted to sit at slightly below eye level to decrease the interpalpebral aperture and exposure. Room humidifiers may be beneficial in dry climates and high altitudes. Moisture chamber eyeglasses can reduce tear evaporation and maintain high humidity around the eye. Nocturnal lagophthalmos can be treated with swim goggles, taping the eyelids closed, or performing a lateral tarsorrhaphy. Patients should be encouraged to eat a balanced diet, rich in n-3 polyunsaturated fatty acids from fish and low in saturated n-6 fatty acids.10 Smoking has been identified to destabilize the tear film and should be stopped.11 Artificial tears are considered a first-line therapy for dry eye. They increase tear volume, minimize desiccation and lubricate the ocular surface. They often provide temporary relief of irritation symptoms in many dry eye conditions. There are a variety of commercially available artificial tears, that contain various agents (Table 12.2) that increase their viscosity, lubricity, retention time and adhesion to the ocular surface. Certain artificial tear formulations contain electrolytes or ions, such as potassium and bicarbonate ions, that are found in normal tears. Tears with a lipid component, such as castor oil (Refresh Optive™ ADVANCED, Systane® Balance, and Soothe® XP) may retard tear evaporation and prevent intrusion of irritating skin lipids. Table 12.2 Composition of Artificial Tears Artificial tears lubricate the ocular surface, reduce tear osmolarity and protect the ocular surface from desiccation. They often provide temporary improvement in eye irritation and blurred vision symptoms, visual contrast sensitivity, tear break-up time, corneal surface regularity and ocular surface dye staining. They have not been found to reverse conjunctival squamous metaplasia.12–19 Benzalkonium chloride is known to disrupt tight junctions and accelerate desquamation of the apical epithelial layer of the cornea in a dose-dependent fashion.20 BAC has detrimental effects on cell membrane integrity and viability. BAC was found to promote apoptosis at lower concentrations and necrosis at higher concentrations following treatment of a conjunctival epithelial cell line.21 It has also been found to stimulate production of inflammatory cytokines (IL-1 and TNF-α) by cultured ocular surface epithelial cells.22 Punctal occlusion should be considered for patients with aqueous tear deficiency and low tear volume. Punctal occlusion is a simple and practical method for conserving endogenously produced tears or instilled artificial tears, increasing tear volume and decreasing tear osmolarity. Punctal occlusion has been reported to decrease ocular irritation symptoms, to improve ocular surface dye staining, and to decrease dependence on artificial tears.23–27 It should be used with caution in patients with normal aqueous tear production (Schirmer 1 scores > 10 mm) and poor tear clearance or in patients with overt lid or ocular surface inflammation, such as meibomian gland disease or ocular rosacea. In these cases, ocular surface inflammation should be controlled prior to punctal occlusion. Dissolvable intracanalicular plugs (lasting 7–10 days for collagen and up to 3 months for synthetic polymers) can be placed into the canaliculis on a trial basis, to determine the efficacy and tolerability of punctal occlusion prior to placement of semipermanent plugs or permanent occlusion. Reversible punctal occlusion can be accomplished with a variety of ‘semipermanent’ dumbbell-shaped silicone plugs that are inserted into the punctal orifice. These plugs are available in a variety of sizes ranging in diameter from 0.4 to 0.8 mm and a gauge can be used to determine the size of the punctum prior to insertion. Silicone plugs are typically retained for weeks to years and have a reported extrusion rate of approximately 7% at 1 month, increasing to 37% at 6 months.28 They can be easily removed with forceps. They are generally well tolerated, but occasionally patients will experience discomfort from the head of the plug rubbing against the medial bulbar conjunctiva. There is also a small risk of pyogranuloma formation at the punctal opening and migration of the plug into the lacrimal canaliculus, that may require surgical removal of the displaced plug.
Treatment of Dry Eye Disease
Introduction
Diagnostic Classification of Dry Eye
Environmental Modification
Artificial Tears
Viscosity Enhancing Agent
Concentration
Found in Commercial Brands
Cellulose derivatives [carboxymethylcellulose (CMC), hydroxypropylmethylcellose (HPMC)]
0.2–1%
Refresh Tears, TheraTears® (CMC); Bion® Tears, Tears Naturale®, Visine®, GenTeal®, Artelac® (HPMC)
CMC + glycerin
0.5-0–9
Refresh Optive™
Polyols [polyethylene glycol (PEG), propylene glycol, glycerin]
0.25–1%
Systane®, Systane Ultra®, Soothe® Lubricant preservative free, Advanced Eye Relief®, Oasis®
Polyvinyl alcohol (PVA)
1–1.4%
HypoTears®, Akwa Tears®, Tears Again®, Tears Naturale® PM, Freshkote
Hyaluronic Acid
0.1–0.18%
Blink Tears®, Hyalistil™ Oasis®, Vismed®
Oil-based emulsions (mineral and castor oil)
Solutions: Refresh Optive™ ADVANCED, Systane® Balance, Soothe® XP Emollient, Ointments: AKWA Tears, LACRI-LUBE®, Systane Nighttime Ointment®,Tears Naturale® PM, REFRESH PM®
Punctal Occlusion
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine