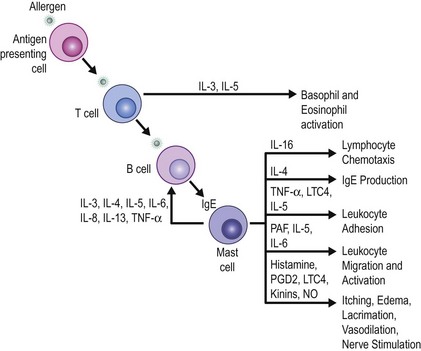
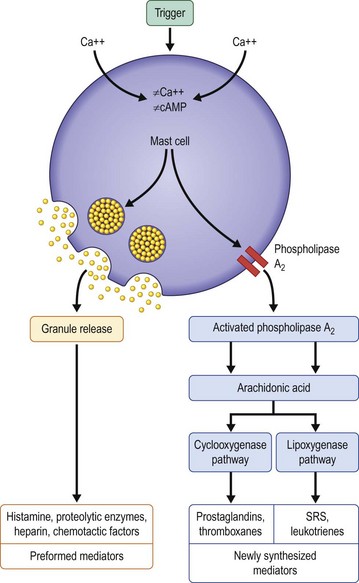
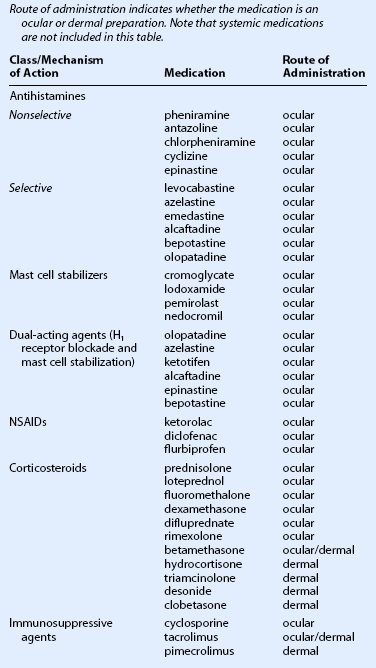
17 SAC is the most prevalent form of ocular allergy and is often accompanied by seasonal allergic rhinitis. Its seasonal incidence is closely tied to the cyclic release of environmental plant-derived airborne allergens. PAC is more likely to occur year-round, though most patients also experience seasonal exacerbations, and is thought to be caused by indoor allergens, such as animal dander and dust mites. Both SAC and PAC can cause significant morbidity, but rarely cause permanent visual impairment. VKC is a less common, self-limited variant of ocular allergy, that can present with unique corneal and conjunctival manifestations, described elsewhere in this text. AKC is a chronic condition associated with atopic dermatitis or eczema, often in individuals with a history of atopy. Both VKC and AKC are primary conjunctival disorders that can cause secondary corneal scarring and therefore, can be vision-threatening. Giant papillary conjunctivitis (GPC) is a reversible condition, most commonly associated with chronic mechanical irritation from contact lenses, exposed sutures, or prostheses. CAC occurs after sensitization to ocular medications and their preservatives.1 Avoiding known allergen triggers is critical to prevent or ameliorate the symptoms of ocular allergies. Many patients are aware of their allergen triggers, but in some cases allergy testing can be helpful. Possible strategies for avoiding allergens include, staying indoors during high pollen counts, using air conditioners and air filters in the home and car, keeping windows closed, and washing hair and clothes after being outdoors. Patients with perennial allergic conjunctivitis may benefit from covering bedding with plastic covers, removing carpets, and avoiding pets. At a minimum, pets should not be allowed in the bedroom. When eyes itch, the natural response is to rub. The temporary relief of itching achieved from rubbing is negated by a more exuberant inflammatory response.2 Eye rubbing may bring large quantities of allergens in direct contact with the conjunctiva from the hands and may mechanically disrupt cell membranes, resulting in further release of inflammatory mediators.2,3 The inflammation, in turn, may result in an itch – rub cycle that is difficult to break. In addition, chronic eye rubbing has been associated with the development of keratoconus. Encouraging patients to stop rubbing their eyes should be a fundamental goal. Cool artificial tears may provide some relief by diluting both inflammatory mediators and allergens on the ocular surface. Cool compresses and ice packs to the eyelids may reduce swelling and provide some additional relief. For many patients, non-medical treatments alone are not sufficient.1 When choosing a medical therapy for allergic conjunctivitis, it is important to remember that the efficacy of an individual medication will vary between patients. As discussed below, each medical therapy targets different mediators in the inflammatory cascade for allergic conjunctivitis (Figs 17.1, 17.2). Selection of an antiallergy medication should be based on the severity, symptoms and projected duration of a patient’s allergic disease. For example, a patient with a severe allergic response may initially benefit from a topical corticosteroid, while a patient with moderate symptoms from complex allergies or who requires extended treatment, may do well with mast cell stabilizers or dual-action agents (mast cell stabilizer/antihistamine). Topical medications are listed in Table 17.1. Table 17.1 Topical Medications for the Treatment of Allergic Conjunctivitis (From Mishra GP, Tamboli V, Jwala J, et al. Recent patents and emerging therapeutics in the treatment of allergic conjunctivitis. Recent Pat Inflamm Allergy Drug Discov 2011;5:26–36.) Over-the-counter topical decongestants containing vasoconstrictors with or without antihistamines are generally well tolerated and effective for patients with mild allergic symptoms.4,5 Although the antihistamine component is weak, the vasoconstrictor component is very effective in reducing conjunctival hyperemia via alpha adrenoceptor stimulation. In the United States, either pheniramine or antazoline, the common antihistamines, is combined with naphazoline, a vasoconstrictor. Using these drops over time may result in tachyphylaxis, requiring patients to use the drops more frequently to obtain the same vasoconstrictor effect. Furthermore, discontinuation of vasoconstricting eyedrops may result in rebound hyperemia.6 Depending on the underlying condition, artificial tears, corticosteroid drops, or long-term therapy with mast cell stabilizers and/or immunotherapy may help alleviate dependence on the vasoconstricting eyedrops.6 Due to their mydriatic effect, topical decongestants are contraindicated in patients with narrow angles. Second-generation antihistamines do not cross the blood – brain barrier. They selectively block peripheral H1 receptors, reducing the occurrence of sedation while still effectively treating allergic symptoms. These more potent topical antihistamines include levocabastine hydrochloride 0.05% and emedastine difumarate 0.05%. Most of the recent antihistamines have also been shown to have some mast cell stabilizing properties as well. Most topical antihistamines have a rapid onset of action, but have a short duration of action, requiring up to four times daily dosing. Selective antihistamines with mast cell stabilizing properties, such as olopatadine, azelastine, ketotifen, alcaftadine, epinastine, and bepotastine, have been shown to have a rapid onset but a longer duration of action when compared to the other topical antihistamines, lasting up to 16 hours.7–10 Because of the improved efficacy of combined antihistamine/mast cell stabilizers, the pure antihistamine drops have largely been replaced by combination drops. Systemic therapy with oral antihistamines (diphenhydramine, carbinoxamine, clemastine, chlorpheniramine, brompheniramine, oxatomide, cetirizine, levocetirizine, loratadine, desloratidine, ketotifen, and fexofenadine) may be beneficial for perennial, vernal, or atopic allergic keratoconjunctivitis, given the chronicity of the disease and the potential for patients to become sensitized to preservatives in some commercial topical preparations. However, oral antihistamines are seldom used to treat isolated seasonal or perennial allergic conjunctivitis, but are frequently used to treat systemic allergy. They should be used with caution in patients with cardiac arrhythmias, or in combination with erythromycin, ketoconazole, itraconazole and troleandomycin. These medications may improve systemic symptoms, but ocular symptoms may worsen. Symptoms of dry eye may be induced or compounded by the propensity of antihistamines to reduce tear production. Topical antihistamines have muscarinic binding properties which, in theory, may also cause or worsen dry eye syndrome. The data on their effect on tear production are conflicting.11 In general, there is little clinical evidence that topical antihistamines induce dryness. When oral antihistamines are needed to treat rhinitis, the addition of a topical antihistamine may help the ocular symptoms. Given that these medications inhibit the release of histamine rather than block histamine receptors, they are better at preventing than treating allergic signs and symptoms. Their effects may not be seen until 2 to 5 days after initiation of therapy, while their maximum benefit is achieved 15 days after initiating therapy. Therefore, if patients have allergic symptoms during a defined season, they should begin these medications about 2 weeks prior to their allergy season and continue throughout the entire season. Mast cell stabilizers represent the mainstay of therapy for vernal and atopic keratoconjunctivitis. Nedocromil, originally thought to be just a mast cell stabilizing agent, is recognized to have multiple actions resulting in rapid relief of symptoms. These actions include antihistaminic (H1 antagonist) effects, reduction of ICAM-1 expression, and inhibitory effects on eosinophils and neutrophils.12 Numerous studies have demonstrated the safety and effectiveness of cromolyn sodium, nedocromil, lodoxamide, and pemirolast, in treating signs and symptoms of vernal and seasonal allergic conjunctivitis.13–21 When comparing the older agents, lodoxamide is about 2500 times more potent than sodium cromoglycate in an animal model, although their efficacy in controlling the symptoms of allergic conjunctivitis is similar.22 A long-term comparison of nedocromil versus cromolyn sodium found that nedocromil 2% produced a more rapid and marked improvement in symptoms over cromolyn 2% and decreased the need for steroid rescue.23 Lodoxamide 0.1% may have additional benefits over cromolyn sodium because it has been found to also have potential antieosinophil action.16,24 Additional studies suggest that mast cell stabilizers may act through other mechanisms. Cromolyn sodium reportedly inhibits the chemotaxis, activation, degranulation, and cytotoxicity of neutrophils, eosinophils, and monocytes.16,25 Lodoxamide and cromolyn sodium may also have effects on Th2 cells, which have been implicated in the pathogenesis of VKC.26 In some patients, mast cell stabilizing drops may be more effective for chronic therapy than dual-acting agents (antihistamine/mast cell stabilizing agents). The dual-acting medications, including olopatadine hydrochloride 0.1% and 0.2%, azelastine hydrochloride 0.05%, ketotifen fumarate 0.025% (available over the counter), alcaftadine 0.25%, bepotastine 1.5%, and epinastine hydrochloride 0.05%, have antihistamine and mast cell stabilizing properties. Most of these drugs have additional modes of action, including eosinophil and basophil inhibition.27,28 These medications are usually effective for the treatment and prevention of signs and symptoms of allergic conjunctivitis.29–31 Olopatadine 0.2% and alcaftadine are the only antiallergy eyedrops approved for once-daily dosing. These dual-action medications are appropriate choices for patients with acute seasonal exacerbations, as well as those with chronic perennial symptoms; they are the mainstay of therapy for the majority of patients with allergic conjunctivitis. Ketorolac tromethamine 0.5%, diclofenac, and flurbiprofen are nonsteroidal anti-inflammatory agents which decrease the activity of cyclooxygenase, an enzyme responsible for arachidonic acid metabolism. The inhibition of cyclooxygenase, in turn, reduces prostaglandin production, most notably the highly pruritic PGE2 and PGI2.32 These drugs have been shown to reduce itching, ICAM-1 expression, and tryptase levels in tears associated with ocular allergy.33–35 Topical ketorolac tromethamine, the only approved nonsteroidal anti-inflammatory drug for managing ocular allergies, has been shown to provide relief of the signs and symptoms of allergic conjunctivitis.36,37 Some patients have transient stinging upon instillation. The newer agents discussed above have largely replaced the topical nonsteroidal anti-inflammatory agents. Signs and symptoms of VKC have been reported to improve with the addition of oral aspirin (1.5 g–4.0 g per day), although routine administration at these high doses could produce serious side effects, especially given that many VKC patients are children.38,39 Topical corticosterioids, including prednisolone, loteprednol, dexamethasone, fluorometholone, and rimexolone, are highly effective for the treatment of ocular allergy because they block most allergic inflammatory cascades (including the late-phase mediators). Corticosteroids diminish the signs and symptoms of ocular allergy by stabilizing capillary permeability, decreasing the influx of inflammatory cells, and inhibiting the activation and degranulation of inflammatory cells.40 Intranasal corticosteroids, when used to treat allergic rhinitis, may also improve concurrent ocular symptoms.41–43 Corticosteroids are particularly helpful in the treatment of VKC and AKC but are less often used for GPC or SAC. Given their propensity to induce cataracts, elevate intraocular pressure in susceptible individuals and potentiate ocular infections, their judicious use is indicated.44 It may be necessary to use corticosteroids in SAC for short periods, if the allergic response is severe and conservative therapy has failed. Loteprednol, an ester corticosteroid which is metabolized in the aqueous humor, is effective in treating seasonal allergic conjunctivitis. In a recent retrospective study, loteprednol 0.2% was well tolerated with no reports of adverse reactions in patients treated for SAC or PAC for at least 12 months.45 Moderate to severe cases of VKC or AKC that are unresponsive to mast cell stabilizers and antihistamines, may necessitate the short-term use of topical corticosteroids. Corneal involvement at any stage warrants the consideration of corticosteroid therapy. Bonini and colleagues reported that 85% of patients in their long-term cohort of 195 VKC patients, required steroids at some point during the course of the disease.46 Allansmith found that ‘pulse’ therapy with topical dexamethasone (1%) given every 2 hours, eight times daily and gradually tapered over days to weeks, to be effective for breakthrough attacks of VKC inflammation.47 In the absence of corneal involvement, low-absorption corticosteroids, such as fluorometholone, loteprednol, and rimexolone, should be tried first. Dose and frequency are determined based on the level of inflammation, with a gradual taper occurring over 2 weeks. Only after first-line therapy fails should more potent agents, such as prednisolone, dexamethasone, or betamethasone be considered.48
Treatment of Allergic Eye Disease
Introduction
Avoidance
Medical Therapy
Vasoconstrictors
Antihistamines
Mast Cell Stabilizers
Dual-Acting Agents
Nonsteroidal Anti-inflammatory Drugs (NSAIDs)
Corticosteroids
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Treatment of Allergic Eye Disease