Chapter 29 Traumatic Facial Paralysis
The course of the nerve from the brainstem to the facial musculature can be divided into three segments: intracranial, intratemporal, and extratemporal or peripheral (Fig. 29-1). The pathophysiology of facial nerve disorders varies according to the segment of the nerve involved. Each segment is discussed individually.

INTRATEMPORAL INJURY TO THE FACIAL NERVE
The intratemporal facial nerve, extending from the internal auditory canal fundus to the stylomastoid foramen, is frequently damaged from blunt trauma to the skull that leads to temporal bone fracture. Fractures produced by blunt trauma have been traditionally grouped into longitudinal and transverse varieties (Table 29-1), although almost any type of fracture can be encountered. Fractures with the main component parallel to the long axis of the petrous pyramid are classified as longitudinal (Fig. 29-2), whereas fractures perpendicular to the long axis (Fig. 29-5) are classified as transverse. Longitudinal fractures are produced by trauma to the lateral aspects of the skull in the temporoparietal region, and compose 80% of fractures in most series.1 Transverse fractures are produced by trauma to the occipital or frontal regions of the skull, and compose about 20% of fractures. Many fractures are oblique or combine elements of longitudinal and transverse fractures.2 Severely comminuted and complex fractures of the temporal bone are commonly produced by penetrating gunshot wounds of the temporal bone.3
TABLE 29-1 Types of Temporal Bone Fractures
| Longitudinal | Transverse | |
|---|---|---|
| Mechanism | Temporal or parietal blow | Frontal or occipital blow |
| Incidence | 80% | 20% |
| Incidence of facial paralysis | 20% | 50% |
| Type of hearing loss | Conductive | Sensorineural |
| External auditory canal | Torn, bloody | Intact |
| Tympanic membrane | Perforated | Intact, hemotympanum |
| Ossicular damage | Common | Uncommon |
| Vertigo | Uncommon | Common |
| Skull base foramen | Ovale | Spinosum, lacerum |
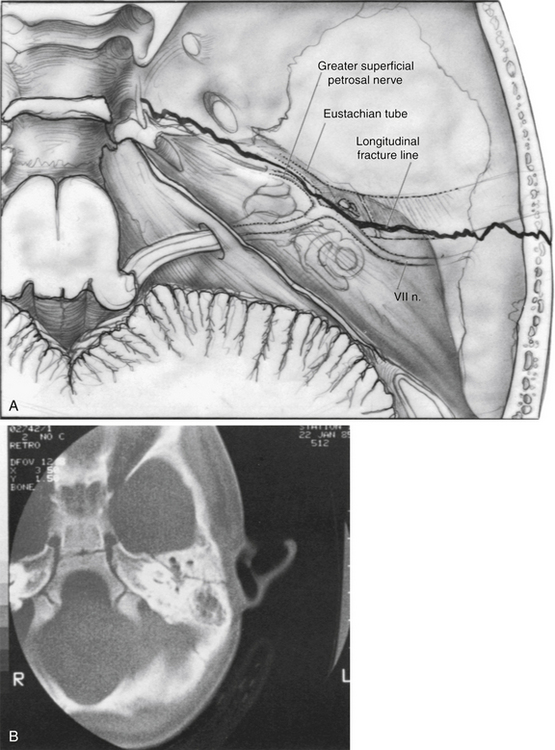
A longitudinal fracture (Figs. 29-2 and 29-3) is suspected when a step-off is present in the external auditory canal and is frequently accompanied by blood in the external auditory canal. A perforation or tear of the tympanic membrane may be present, and cerebrospinal fluid (CSF) otorrhea is occasionally seen. Sterile instruments should be used during the examination of the external auditory canal to avoid introducing contamination into the area and producing retrograde meningitis. A conductive hearing loss usually is present and can have numerous causes. Perforation of the eardrum, hematoma in the middle ear cleft, disruption of ligaments supporting the ossicles in the attic region, and disruption of the ossicular joints all can lead to varying degrees of conductive hearing loss (see section on ossicular damage).
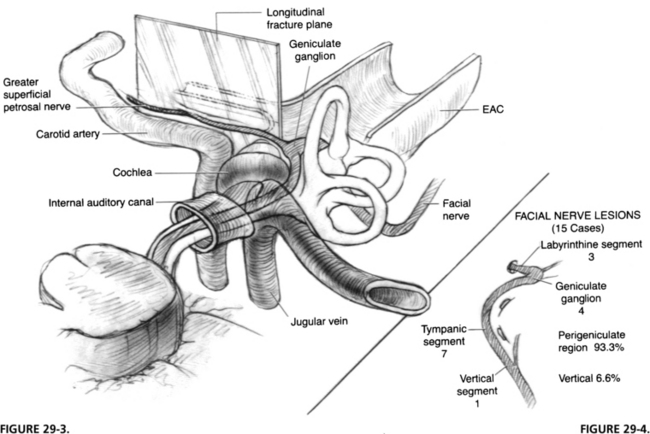
FIGURE 29-3 Longitudinal fracture of temporal bone. EAC, external auditory canal.
FIGURE 29-4. Location of lesion to facial nerve in 15 cases of longitudinal fractures.
(From Coker NJ, Kendall KA, Jenkins HA, Alford BR: Traumatic intratemporal facial nerve injury: Management rationale for preservation of function. Otolaryngol Head Neck Surg 97:262-269, 1987.)
A longitudinal fracture often extends to the foramen ovale. Facial paralysis is seen in only 20% of longitudinal fractures, but is the most common cause of facial paralysis in blunt trauma of the temporal bone because of the relative infrequency of transverse fractures. The facial nerve is involved in the perigeniculate region in 90% of cases4,5 and less commonly in the mastoid segment by fractures of the posterior external auditory canal (Fig. 29-4). The pathology of the facial nerve injury in blunt temporal bone trauma, in decreasing order of occurrence, consists of intraneural hemorrhage, bony fragment impingement, and nerve transection.6
A transverse temporal bone fracture is suspected when a patient presents with sensorineural hearing loss and vertigo accompanied by facial paralysis. The external canal is frequently intact, and no evidence of canal wall discontinuity and hemotympanum may be present (Figs. 29-5 and 29-6). Transverse fractures can extend into the foramen spinosum or lacerum. These patients have a 50% incidence of facial paralysis, which occurs from damage to the geniculate ganglion region (Fig. 29-7).7 The causes of injury are the same as for longitudinal fractures, and intraneural hemorrhage is the most common.


FIGURE 29-6 Transverse fracture of temporal bone. EAC, external auditory canal.
FIGURE 29-7. Location of lesion in three cases of transverse temporal bone fracture.
(From Coker NJ, Kendall KA, Jenkins HA, Alford BR: Traumatic intratemporal facial nerve injury: Management rationale for preservation of function. Otolaryngol Head Neck Surg 97:262-269, 1987.)
The traditional classification scheme, based on anatomic cadaveric studies performed more than 50 years ago,8 has been criticized because of its inability to predict complications of temporal bone fractures. More recently, several authors have proposed new classification schemes with predictive ability.9–12 These schemes are similar and are based on whether the otic capsule or petrous apex or both are violated. Fractures involving the otic capsule were significantly more likely to result in the complications of facial nerve injury, sensorineural hearing loss, and CSF leak than fractures that did not. The new classification systems seem to have utility for predicting these serious sequelae of temporal bone fractures.
Gunshot wounds to the temporal bone region typically produce extensive damage, the degree of which is determined by the velocity of the projectile. Low-velocity civilian projectiles have low energy and produce mainly locally destructive manifestations. In contrast, high-velocity, large-caliber weapons, which are increasingly being seen on city streets, are capable of widespread destruction, with extensive local and regional manifestations produced by the concomitant shock wave. Severe life-threatening injuries including vascular and intracranial damage are seen in one third to one half of patients and must be stabilized first. Angiography and computed tomography (CT) scan of the head are needed as part of the initial evaluation.13,14
In gunshot wounds to the temporal bone, the incidence of facial nerve injury is about 50%, with the vertical segment being the most frequently damaged.3,13 Less frequent sites of injury include the tympanic segment, the main trunk just distal to the stylomastoid foramen, and the labyrinthine segment. At the time of surgery, two thirds to three fourths of patients were found to have complete transection of the facial nerve13; interposition grafts and transmastoid decompression have been the primary modalities of treatment. Because residual bullet fragments can remain lodged in the temporal bone and can become a nidus for infection, a canal wall down or radical mastoidectomy has been advocated as the approach of choice.13,15 Gunshot wounds of the temporal bone frequently result in loss of a segment of the nerve, usually in the vertical portion, requiring interposition grafting for repair. There is also a high incidence of concomitant vascular and central nervous system injuries.
PATIENT EVALUATION
The presentation of facial nerve injuries greatly affects their management. The presence of a tightly enclosing fallopian canal around the intratemporal facial nerve makes the nerve much more susceptible to all types of trauma. Lack of any space to accommodate edema, which inevitably accompanies soft tissue trauma, leads to further neural injury. An injured nerve may not manifest significant clinical dysfunction initially, but later, after sufficient edema has occurred to prevent axoplasmic flow, the injury manifests. Fisch6 and others16–18 have shown that the area of the fallopian canal with the least expansion room for neural swelling is in the region of the meatal foramen. Because most injuries to the facial nerve occur in the perigeniculate area just distal to the meatal foramen, the edema produced in facial nerve injury is quite critical in the pathophysiology of this disorder.
The findings elicited from a careful history and physical examination on the patient’s presentation to the emergency department provide prognostic data and determine appropriate management. Eyewitness accounts of facial nerve function immediately after the injury and of any progression during transport to the emergency department are often unreliable and likely to be fraught with inaccuracy, but still can provide important information, especially if an initial examination is impossible because of other life-threatening injuries. An accurate analysis of facial nerve function might be impossible if the patient has been intubated and sedated as part of the primary survey, but every effort should be made to elicit some sort of facial movement, even a grimace, in a comatose patient. Patients with any facial movement after the injury and before the onset of paralysis rarely need surgical intervention.19 A nerve with diffuse weakness in all branches can be observed clinically, and if some function persists, expectant management can be employed. If this situation deteriorates to total paralysis, electric testing should be used to follow the nerve to ensure that total degeneration does not occur.
Audiometric evaluation should also be performed as soon as the patient’s condition permits. The type of hearing loss can corroborate CT scan findings. If surgical exploration is warranted, the severity of the hearing loss in the affected ear guides the surgeon in determining the best approach,19–21 and serves as a baseline with which to compare postoperative results.22
Prognosis Based on Electric Studies
Fisch23 and Esslen16 have postulated that surgery can facilitate return of facial nerve function if performed before complete degeneration. A level of 90% degeneration or less, as determined by electroneuronography (ENoG), has been correlated with a uniformly good prognosis for return of function. If the nerve is nonfunctional at the initial examination, the chance of a complete transection is high and will likely require surgery.
Patients with complete facial paralysis at the initial examination are screened daily with nerve excitability testing. This test uses direct transcutaneous stimulation of the nerve on each side of the face and determines a stimulation threshold that produces perceptible movement. The normal side is used as a control. If the threshold difference between the normal and dysfunctional sides exceeds 2.5 mA, ENoG is performed regularly thereafter. ENoG uses transcutaneous supramaximal stimulation of the facial nerve while recording the evoked potential from anterograde stimulation in the periphery of the face.24 The maximal evoked response of the nerve is measured on each side by use of a nonfixed recording electrode technique. A side-to-side comparison is made, with the normal side serving as the control. The percentage of degeneration is calculated as the difference between the two sides. More recent data have shown that a correlation exists between ENoG and nerve excitability testing: a 90% degeneration score on ENoG correlates to about a 3.5 mA difference on nerve excitability testing.25
Chang and Cass,26 in a comprehensive and critical assessment of the available literature on facial nerve injury secondary to temporal bone trauma, proposed that serial ENoG be performed in any patient with acute-onset complete facial nerve paralysis or acute-onset incomplete paralysis that subsequently progresses to complete paralysis. Only patients progressing to greater than 95% degeneration within 14 days are at risk for poor outcomes and should be offered facial nerve exploration. Patients with incomplete paralysis at presentation who do not progress to complete paralysis and patients who have a normal initial examination with subsequent delayed-onset facial nerve paralysis, whether complete or not, have an excellent prognosis for recovery and can be observed.
In a nonacute injury, ENoG can be relied on for up to 3 weeks, but after this period, a desynchronization (deblocking) of electrically evoked facial nerve discharge can occur, preventing a single unified discharge of all neurons in the trunk. This effect occurs because of the differing time courses over which recovering neurons re-establish electric conductivity and the capability to conduct an action potential. At this stage, it is no longer possible to compare the diseased, asynchronously discharging side with the unaffected, synchronously discharging side, making accurate determination of the severity of degeneration by this technique alone impossible. If by 3 weeks after injury the patient has not progressed to 90% degeneration, however, it is unlikely surgery would be needed.26
After 3 weeks, electromyography (EMG) may be used to establish whether recovering axons are present. This information is useful if delayed intervention is being considered. Voluntary motor units and polyphasic potentials indicate that regeneration is in progress. Lack of the foregoing and fibrillation potentials indicate a fully degenerated nerve without evidence of ongoing recovery. EMG can detect signs of wallerian degeneration, such as fibrillation potentials, only after the 10th day following nerve injury.6,7,21 A limitation of EMG is that it cannot be used initially following injury; however, it does not seem to have the reliability and reproducibility issues that several authors have found with ENoG.27,28



